Ok jumping back on because it’s been a while. Been running 100mg spread over two doses every 3.5 days (60/40 mg) since I last posted. Been feeling ok, steady. Wondering if dose could go up. Couple things here. Got labs back yesterday (all except E2, Sensitive test takes longer) . I’ve got a two part
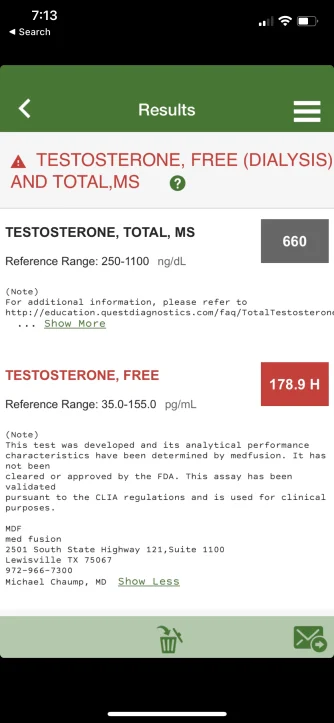
total test - 660
Free test - 179
SHBG - 15
thoughts on increasing to 120mg week?
2nd question - after 4 month waiting period I did go see Dr. Larry Lipshultz in Houston and he’s recommending I start on 200mg week injected once weekly with a 1mg dose of anastrozole per week. I have to admit I was shocked to hear him say this, that doesn’t seem like the right step considering he is supposed to be a leader in the field. Any thoughts on him / his recommendation?
Not sure why you are splitting your dose T 100 mg/week (60/40) as it will make no difference and I would just stick with 50 mg every 3.5 days.
Have no idea where your FT level truly sits as you did not post-lab reference ranges let alone the testing method used.
As I have stated numerous times on the forum that although TT is important to know FT is what truly matters as it is the active unbound fraction of testosterone responsible for the positive effects.
The only way to know where your FT level truly sits is to have it tested using the most accurate assays such as the gold standard Equilibrium Dialysis or Ultrafiltration.
If these are labs at the trough and you are hitting a TT 660 ng/dL and SHBG sits at 15 nmol/L than your FT levels would be descent and something you need to keep in mind is that your peak levels will be much higher.
If you feel well overall and blood markers are healthy then you can either leave it be or try increasing your dose slightly if you feel that there is room for improvement.
Forget the 200 mg/week protocol with the added AI.
Such dose will have your TT/FT level through the roof let alone the peak--->trough will be extreme and can have a negative impact on energy/mood/libido/erections.
Top it off that your SHBG 15 nmol/L is on the lower end.
You already tried a higher dosed T protocol and it did not work out so well.
On your current protocol of 100 mg/week split 60/40 every 3.5 days you are hitting a robust trough TT almost 700 ng/dL let alone FT level will be descent as your SHBG is on the lower end.
Keep in mind that increasing your dose T from 100--->120 mg/week may not seem like a big jump that 20 mg esterified T will most likely drive your trough TT >1000 ng/dL let alone have your FT very high as you have low SHBG.