Hey there,
I’ve been following the various threads on Prop / blends for some time and have had a similar journey as
@Cataceous (low shbg, cypionate kryptonite, e2 sensitivity etc). I do have pubertal gyno which I’m planning to have removed later in the year - and suspect this plays a role.
I’ve been on Test / AAS for about 5 years and was always fine on low dose Test with Higher tren (but modest dose) for periods of time, always struggled with trying to be on Test-only. Orals never worked consistently enough.
And of course Tren forever is absolutely not sustainable due to other levels going out of whack.
I’ve been through all the usual rollercoasters too with AIs and what not.
Just wanted to share my guinea pig experiment incase it’s useful to the community.
So.. where I’m at is that 3-5mg of Prop works very nicely, with a raging libido for the first part of the day but the trough is a bit too deep.
And..what I am presently experimenting with is 0.04ml Sustanon at 15:00 each day, with 2mg of prop in the evening before bed.
I am using Hcg although I haven’t quite found the right dose, in a sense that I can’t tell much difference, but for belts and braces I’m doing 520 iu EOD (Omnidrel).
I’ve felt consistent the last week or so but need to see if the longer esters creep up on me again as seems to always be the case. For most of my time on TRT/AAS I’ve preferred Test Phenylprop which has a more mid range half life but still compounds and peaks my e2 too high so I end up having to skip / reset.
If I throw daily Tren Ace back in on a minimal dose (30mg/week) of Phenylprop im fine.
For completeness I’ve been on Lexapro 10mg for years (no sexual sides), and I take Cialis 5mg / day, sometimes up to 20mg if it’s date night. SHBG at last test was 11 (up from 8) since starting the dailies.
I’ve had my fair share of embarrassing moments when I’ve needed to perform so hope someone finds my posts useful.
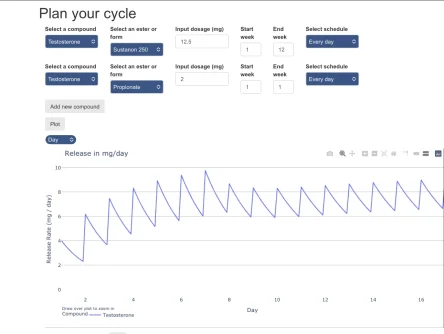
Edit; added a chart of the protocol from the start where I used prop to “bridge” my levels until steady state. This is helpful from a psychological perspective and getting out of the “nothing works” rut when trying to do longer esters daily - so you can at least enjoy yourself a bit and get your confidence back.
To lower my E2 levels and flush everything about before this, I went cold turkey and used Vitamin D at 2000IU/day. I took bloods every 3 days over two weeks before starting pinning again.
My e2 was at 196 pmol/l at that particular peak when I was feeling “good” and subsequently crashed from further pinning (was on around 70mg/week split into two doses) and is now around 114 pmol/l and will likely have risen favourably by my next test.
My emphasis is on E2, not because it’s “bad” but because of the “sweet spot” and being particularly sensitive to it.