
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
So who is happy with TRT? Who wish they never started?
- Thread starter 42HRT
- Start date
-
- Tags
- testestone


Vince
Super Moderator
16 mg of testosterone cypionate daily, 500 iu of hcg twice weekly and no AI.@Vince thank you. What ester and dosage are you using? Where is your total t levels?
Pregnenolone 10 mg and 25 mg of DHEA.
My last injection before labs, about 28 hr.s.
Testosterone, Total, LC/MS, 1035.9 High ng/dL 264.0-916.0
Testosterone, Free 33.77 High ng/dL 5.00-21.00
% Free Testosterone 3.26% 1.50-4.20
DHEA-Sulfate01 499.0 High ug/dL 30.9-295.6 age adjust
Dihydrotestosterone 56 ng/dL
Estradiol, Sensitive 18.7 pg/mL 8.0-35.0
Sex Horm Binding Glob, Serum. 41.2 nmol/L 19.3-76.4
Hemoglobin. 16.7 g/dL 13.0-17.7
Hematocrit 47.7 37.5-51.0
tropicaldaze1950
Well-Known Member
No. As on this forum, some men have been on long term daily shots, either IM or subq, after trying other protocols, and have found success. There's a practitioner on there who does a weekly injection and prescribes that for many of his patients, though some have switched to 2X weekly. He prescribes doses between 140 and 200 mg. Some men on the forum micro dose, 50 to 70 mg.@tropicaldaze1950 is there any consensus? I see some evidence the longer acting, has lower effect on lips and RBC's.
tropicaldaze1950
Well-Known Member
I've been following your journey for a few years and it's great that oral T is working! I was reading an abstract on steroidogenesis and the authors stated that oral forms of testosterone closely mimic the daily peaks and troughs of endogenous testosterone.I always wake up in the middle of the night and morning with erections, recently increased sex to a couple of times per week. Desire is always increasing.
I go to the gym every day, 7 days a week, for an hour and a half, then I go to work at Amazon 2 hours later. I still have energy later in the evening.
Co-workers keep asking me if I run out of energy towards the end of my shift, because I’m full throttle the entire time. They call me the machine.
I’ll let you judge, how’s that for energy?
Fasting glucose is 114.
My ferritin is now 198, which was stuck <100 for years.
I looked up the inactive ingredients in Jatenzo and not sure it or any other oral form is for me because of my many chemical sensitivities. I'm a walking disaster in that regard, LOL.
Mixed feelings. I started TRT after Clomid stopped working. I think I started with too high a dose because I had horrible acne and my hair started shedding, which led me to finasteride. Propecia caused severe damage that never fully healed. I wish I had tried adding hCG to Clomid rather than go on TRT.
How long were you on clomid before it stopped working? Was stopped working that your test levels fell again? Did you try upping the dose?Mixed feelings. I started TRT after Clomid stopped working. I think I started with too high a dose because I had horrible acne and my hair started shedding, which led me to finasteride. Propecia caused severe damage that never fully healed. I wish I had tried adding hCG to Clomid rather than go on TRT.
4 years. Yes my test levels dropped to hypogonadal levels (I have empty sella). I tried switching to enclomiphene for 3 months with no success. I wish I had kept trying though. I saw an interview with Dr. Mohit Khera where he said some men who dose Clomid daily will lose efficacy so it should be dosed every other day. I think maybe that happened to me.How long were you on clomid before it stopped working? Was stopped working that your test levels fell again? Did you try upping the dose?
What damage did propecia cause?Mixed feelings. I started TRT after Clomid stopped working. I think I started with too high a dose because I had horrible acne and my hair started shedding, which led me to finasteride. Propecia caused severe damage that never fully healed. I wish I had tried adding hCG to Clomid rather than go on TRT.
Golfboy307
Active Member
Been on it for over 8 years, now age 55. Pre -treatment was in the upper 300's with low free T. Make a huge positive difference for me in all facets. Hope I never have to go off!
madman
Super Moderator
I've been following your journey for a few years and it's great that oral T is working! I was reading an abstract on steroidogenesis and the authors stated that oral forms of testosterone closely mimic the daily peaks and troughs of endogenous testosterone.
I looked up the inactive ingredients in Jatenzo and not sure it or any other oral form is for me because of my many chemical sensitivities. I'm a walking disaster in that regard, LOL.
If anything you are getting 2 daily peak/troughs 24/7.
T levels will be much lower before it is time for your second dose (12 hrs after 1st dose) let alone after you take your second dose you will hit a high Cmax 2-4 hrs later than T levels would rapidly decline and will be much lower overnight until your next dose in the early AM.
Even if dosed once daily which no one would do your T levels would be much lower in the evening/throughout the night until your next morning dose.
Many fail to realize that T levels gradually rise overnight reaching peak in the early AM.
*elevated and near peak TT level during nighttime sleep, peak TT level around the time of morning awakening
*T production occurs in the greatest amount during sleep as recurring pulses at approximately 90 min intervals in healthy young males and approximately 140 min in healthy middle-aged males (91).
This is key:
(i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
*There are substantial differences between the therapies in the derived TT 24 h pattern; moreover, all but one of them differs either somewhat or greatly from the normative one of diurnally active young adult males, which is defined by:
(i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
*The serum TT concentration generated by the Striant® mucoadhesive buccal tablet system applied to the upper gum above the incisor of either side of the mouth twice daily at equal intervals displays 12 h-like patterning, with the Cmax following closely after each application and the overall 24 h Cmin occurring during sleep (Figure 3A).
*The Jatenzo® oral soft gel capsule formulation ingested twice daily at equal intervals also gives rise to variable TT levels of distinct 12 h patterning, with prominent Cmax following 2 to 4 h after each ingestion and rapidly declining levels thereafter (Figure 3B).
*As shown in the graphs of Figures 2 and 3, the PK of most FDA-approved PA-TRTs gives rise to TT 24 h patterns that deviate greatly from the normative one thereby failing to satisfy one or more of the five specified criteria.
*AndroGel® 1%, AndroGel® 1.62%, Xyosted®, and Striant®, which achieve relatively constant serum hormone concentration throughout the 24 h, seem to have been incorrectly conceptualized, perhaps because of the presumed necessity to maintain nonvarying, that is, homeostatic, TT concentration to achieve consistency of biological effects.
*The FDA-approved gel and solution PA-TRTs when applied as directed, that is, morning after awakening from nighttime sleep, while achieving TT levels within the normal range to remedy androgen hormone deficiency, fail to restore the normal physiologic TT circadian variation.
*The temporal patterns of these PA-TRTs differ from normal, either in the timing of the peak and/or nadir TT concentrations, by achieving the highest hormone levels generally between midmorning and noon and lowest (rather than near peak) ones during sleep (Figure 2A-2F).
Does Patient-Applied TRT Pose Risk for Blood Pressure Elevation? - Excel Male TRT Forum
Does Patient-Applied Testosterone Replacement Therapy Pose Risk for Blood Pressure Elevation? Circadian Medicine Perspectives (2022) Michael H. Smolensky, Ramon C. Hermida, Linda Sackett-Lundeen, *Ramon G. Hermida-Ayala, and Yong-Jian Geng ABSTRACT We reviewed medication package inserts, US...
*The US Food and Drug Administration (FDA), since the 1950s, has approved several physician-administered injectables and implantable pellets plus 10 unique (nonbiologically similar) patient-applied (PA) transdermal gel, intranasal gel, transdermal solutions, skin patches, buccal tablet, oral capsule, and subcutaneously injected TRTs. Intramuscularly injected and surgically implanted TRTs are administered by healthcare professionals at intervals of several weeks or months, whereas PA transdermal gel and solutions are dosed once daily at the commencement of the activity period, buccal tablet and oral soft gel capsule two times daily at approximately 12 h intervals, intranasal gel three-times daily at approximately 6 to 8 h intervals, and transdermal patch once daily before bedtime. As subsequently discussed, there is a substantial difference in the pharmacokinetics (PK) and attained T 24 h patterning between the 10 different PA-TRTs.
*LH pulses exhibit 24 h temporal patterning; they occur in greater number and higher amplitude during the sleep than wake span, suggesting the involvement of sleep-facilitating or sleep-dependent processes (10, 17, 57, 164, 175–177). Consequently, T production occurs in the greatest amount during sleep as recurring pulses at approximately 90 min intervals in healthy young males and approximately 140 min in healthy middle-aged males (91).
*Figures 2A-2F depict the TT 24 h pattern achieved by the 6 different solution and gel PA-TRTs, and Figures 3A-3D depict the TT 24 h pattern achieved by the buccal tablet, oral capsule, transdermal patch, and subcutaneously injected PATRTs. There are substantial differences between the therapies in the derived TT 24 h pattern; moreover, all but one of them differs either somewhat or greatly from the normative one of diurnally active young adult males, which is defined by: (i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
AndroGel® 1%, AndroGel® 1.62%, Axiron®, Fortesta®, and Testim® (and its biosimilar Vogelxo®) gel and solution preparations are recommended for application once daily in the morning to attain the highest serum hormone level 2 to 6 h following dosing and lowest, instead of highest, hormone level during sleep, that is, final hours of the 24 h dosing interval (Figure 2A-2E).
The Natesto® gel product applied to each nostril three times daily at approximately equal intervals results in highly variable serum TT concentration during the 24 h, showing three prominent peaks (Cmax), each occurring approximately 40 min after the administrations, and three prominent nadirs (Cmin) of 2 to 4 h duration, each occurring midway through the dosing intervals (Figure 2F).
The serum TT concentration generated by the Striant® mucoadhesive buccal tablet system applied to the upper gum above the incisor of either side of the mouth twice daily at equal intervals displays 12 h-like patterning, with the Cmax following closely after each application and the overall 24 h Cmin occurring during sleep (Figure 3A).
The Jatenzo® oral soft gel capsule formulation ingested twice daily at equal intervals also gives rise to variable TT levels of distinct 12 h patterning, with prominent Cmax following 2 to 4 h after each ingestion and rapidly declining levels thereafter (Figure 3B).
Xyosted®, a patient subcutaneously injected TRT at weekly intervals, has yet to be rigorously evaluated for its TT day-night pattern. Available data based upon rather infrequent blood sampling indicate Cmax occurs approximately 12 h following each weekly administration and that TT is maintained within the therapeutic range in a relatively stable manner, at least throughout the initial days of the 7-day dosing period (Figure 3C).
*The TT concentration produced by the Androderm® transdermal patch applied to the skin of the back, stomach, upper arms, or thighs nightly before retiring to sleep more closely reproduces the normative TT circadian pattern of young adult males than any of the other marketed PA-TRTs. Following application, TT concentration progressively rises during sleep and peaks around the time of morning awakening; it progressively declines during late morning and afternoon, reaching its nadir (Cmin) in the evening before the next scheduled patch application (Figure 3D).
I have been at this way too long!
troughs of natural T? - Excel Male TRT Forum
just curious folks who were borderline low T how much of a difference getting bloods an hour or 2 later in the day? ie are u 400 when woke up and bloods later in the day how much lower did they get? anyway, ive only seen charts of folks with normal T start at 700 and go down to 300 or so...
A pill that could outsell Viagra: New testosterone Rx drug - Excel Male TRT Forum
https://www.americanbazaaronline.com/2022/10/11/testosterone-drug-kyzatrex-hits-market-451261/ Kyzatrex could be a potential blockbuster to treat testosterone deficiency, a severely undertreated disease. Testosterone has been historically perceived as a lifestyle issue for men who want to...
Who Started TRT w/ "Normal" Levels @ What Age? - Page 3 - Excel Male TRT Forum
Latest labs in August were all middle range, slightly lower for my age. I turn 45 tomorrow and I feel fine, mostly, but 'things aren't what they used to be'. All my friends my age are on TRT, and some telling to do 150+ once a week. That seems extreme to me with my numbers...
Official Natesto Thread - Page 5 - Excel Male TRT Forum
Welcome to the Natesto thread. I have used Natesto on an off for several years, but it seems to be one of the less popular TRT options here. That said, I have seen a few readers mention it, and I thought it would be good to start a dedicated thread on Natesto where people can share their...
Gel or inject ? - Excel Male TRT Forum
I have been using T gel for many years, 2 packets of 1% , 50mg /packet / day. I am considering a change to injectable test/cyp, really just for the cost factor. I just moved to medicare and the deductable plus the cost of the gel is pretty high. I am wondering about the cycle of high to low...
Tips on how to blend propionate with enanthate (or cypionate)? - Page 4 - Excel Male TRT Forum
I have been having some success with low dose daily propionate for the last several months. Dose levels have ranged from 8-10 mg injected every morning after waking. Overall, it has been a far better experience than my previous cypionate protocol of 80-100 per week (split every 3.5 days)...
ANDRODERM® (TDS) - Excel Male TRT Forum
https://www.androderm.com/about-androderm ANDRODERM® (testosterone transdermal system) is designed to deliver testosterone continuously for 24 hours following application to intact, non-scrotal skin (e.g., back, abdomen, thighs, upper arms). Four strengths of ANDRODERM® are available that...
Water retention when I inject @ evening and less when @ morning, ideas why ? - Excel Male TRT Forum
I feel the best emotionally and get the best sleep as close to being natty when I inject ED around 12,5mg Test Prop in the evening prior to bed. Been experimenting for quite some time and indeed there is a very big difference. Wake up full of energy and feel calm during the day. Also this...
Best time to inject Test - Evening? - Excel Male TRT Forum
When is the best time of day to inject Test C or HCG? Natural testosterone is highest in the morning so it seems injecting Test in the evening is the best option? Don't have any idea when the best time to inject HCG is.
Still trying to find libido - Page 3 - Excel Male TRT Forum
I’ve been on topical cream (not applied to testicles) and now shots. I was on the 100mg dose of cream and that brought my dht up but not my t. So I switched to shots. I’ve been taking daily shots now for 6 weeks at 150mg per week. My shbg is 15, e2 47, t-778, ft- 159 (max is 155). It seems one...
New thoughts on AI - Excel Male TRT Forum
I was curious if you all have seen some of the latest research, and doctors on YouTube, other forums Etc. advocating to not block estradiol i.e. do not take an AI – and that it is more beneficial and causes no harm to let estrogen reach its own level when on testosterone supplementation. Have...
Applying cream twice a day problems - Excel Male TRT Forum
To those of you applying cream BID, do you have sleep issues after applying the second dose at night. Cream seems to be very activating and I can’t sleep at night when I apply the second dose. If I just apply the morning dose I sleep fine. Anybody else have this issue ?
Creams with new application over injectable? - Excel Male TRT Forum
Hi all - I've heard many problems with creams both here and from other sources. However, this recent Tweet from Dr. Jay Campbell got me curious: Has anyone heard about this? What do you think? They're doing 2x / day application which would theoretically lead to more stable levels...
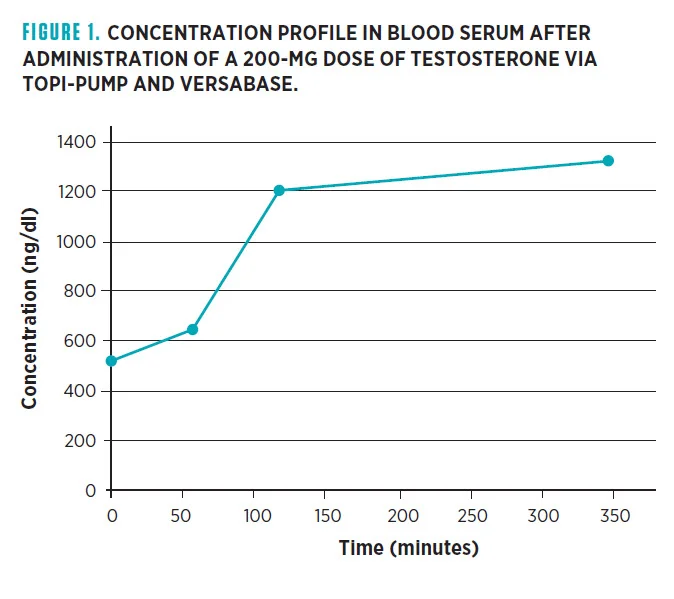
Case Study: Absorption of Testosterone Cream via Scrotal Delivery
Case Study: Absorption of Testosterone Cream via Scrotal Delivery. Needham S1, Needham S2. 1Moses Lake Professional Pharmacy, Moses Lake, Washington. 2Alturas Analytics in Moscow, Idaho. Abstract Transdermal testosterone has been used for years to treat patients with low testosterone...
Systemlord
Member
I would like to see a once daily extended release Jatenzo option, perhaps with similar half-life to Cialis.
It’s only a matter of time.
It’s only a matter of time.
madman
Super Moderator
I would like to see a once daily extended release Jatenzo option, perhaps with similar half-life to Cialis.
It’s only a matter of time.
Lipocine is already ahead of the game!
This is next in line.
*TLANDO XR (Testosterone Tridecanoate)
tropicaldaze1950
Well-Known Member
If anything you are getting 2 daily peak/troughs 24/7.
T levels will be much lower before it is time for your second dose (12 hrs after 1st dose) let alone after you take your second dose you will hit a high Cmax 2-4 hrs later than T levels would rapidly decline and will be much lower overnight until your next dose in the early AM.
Even if dosed once daily which no one would do your T levels would be much lower in the evening/throughout the night until your next morning dose.
Many fail to realize that T levels gradually rise overnight reaching peak in the earl AM.
*elevated and near peak TT level during nighttime sleep, peak TT level around the time of morning awakening
*T production occurs in the greatest amount during sleep as recurring pulses at approximately 90 min intervals in healthy young males and approximately 140 min in healthy middle-aged males (91).
This is key:
(i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
*There are substantial differences between the therapies in the derived TT 24 h pattern; moreover, all but one of them differs either somewhat or greatly from the normative one of diurnally active young adult males, which is defined by:
(i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
*The serum TT concentration generated by the Striant® mucoadhesive buccal tablet system applied to the upper gum above the incisor of either side of the mouth twice daily at equal intervals displays 12 h-like patterning, with the Cmax following closely after each application and the overall 24 h Cmin occurring during sleep (Figure 3A).
*The Jatenzo® oral soft gel capsule formulation ingested twice daily at equal intervals also gives rise to variable TT levels of distinct 12 h patterning, with prominent Cmax following 2 to 4 h after each ingestion and rapidly declining levels thereafter (Figure 3B).
*As shown in the graphs of Figures 2 and 3, the PK of most FDA-approved PA-TRTs gives rise to TT 24 h patterns that deviate greatly from the normative one thereby failing to satisfy one or more of the five specified criteria.
*AndroGel® 1%, AndroGel® 1.62%, Xyosted®, and Striant®, which achieve relatively constant serum hormone concentration throughout the 24 h, seem to have been incorrectly conceptualized, perhaps because of the presumed necessity to maintain nonvarying, that is, homeostatic, TT concentration to achieve consistency of biological effects.
*The FDA-approved gel and solution PA-TRTs when applied as directed, that is, morning after awakening from nighttime sleep, while achieving TT levels within the normal range to remedy androgen hormone deficiency, fail to restore the normal physiologic TT circadian variation.
*The temporal patterns of these PA-TRTs differ from normal, either in the timing of the peak and/or nadir TT concentrations, by achieving the highest hormone levels generally between midmorning and noon and lowest (rather than near peak) ones during sleep (Figure 2A-2F).

Does Patient-Applied TRT Pose Risk for Blood Pressure Elevation? - Excel Male TRT Forum
Does Patient-Applied Testosterone Replacement Therapy Pose Risk for Blood Pressure Elevation? Circadian Medicine Perspectives (2022) Michael H. Smolensky, Ramon C. Hermida, Linda Sackett-Lundeen, *Ramon G. Hermida-Ayala, and Yong-Jian Geng ABSTRACT We reviewed medication package inserts, US...www.excelmale.com
*The US Food and Drug Administration (FDA), since the 1950s, has approved several physician-administered injectables and implantable pellets plus 10 unique (nonbiologically similar) patient-applied (PA) transdermal gel, intranasal gel, transdermal solutions, skin patches, buccal tablet, oral capsule, and subcutaneously injected TRTs. Intramuscularly injected and surgically implanted TRTs are administered by healthcare professionals at intervals of several weeks or months, whereas PA transdermal gel and solutions are dosed once daily at the commencement of the activity period, buccal tablet and oral soft gel capsule two times daily at approximately 12 h intervals, intranasal gel three-times daily at approximately 6 to 8 h intervals, and transdermal patch once daily before bedtime. As subsequently discussed, there is a substantial difference in the pharmacokinetics (PK) and attained T 24 h patterning between the 10 different PA-TRTs.
*LH pulses exhibit 24 h temporal patterning; they occur in greater number and higher amplitude during the sleep than wake span, suggesting the involvement of sleep-facilitating or sleep-dependent processes (10, 17, 57, 164, 175–177). Consequently, T production occurs in the greatest amount during sleep as recurring pulses at approximately 90 min intervals in healthy young males and approximately 140 min in healthy middle-aged males (91).
*Figures 2A-2F depict the TT 24 h pattern achieved by the 6 different solution and gel PA-TRTs, and Figures 3A-3D depict the TT 24 h pattern achieved by the buccal tablet, oral capsule, transdermal patch, and subcutaneously injected PATRTs. There are substantial differences between the therapies in the derived TT 24 h pattern; moreover, all but one of them differs either somewhat or greatly from the normative one of diurnally active young adult males, which is defined by: (i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
AndroGel® 1%, AndroGel® 1.62%, Axiron®, Fortesta®, and Testim® (and its biosimilar Vogelxo®) gel and solution preparations are recommended for application once daily in the morning to attain the highest serum hormone level 2 to 6 h following dosing and lowest, instead of highest, hormone level during sleep, that is, final hours of the 24 h dosing interval (Figure 2A-2E).
The Natesto® gel product applied to each nostril three times daily at approximately equal intervals results in highly variable serum TT concentration during the 24 h, showing three prominent peaks (Cmax), each occurring approximately 40 min after the administrations, and three prominent nadirs (Cmin) of 2 to 4 h duration, each occurring midway through the dosing intervals (Figure 2F).
The serum TT concentration generated by the Striant® mucoadhesive buccal tablet system applied to the upper gum above the incisor of either side of the mouth twice daily at equal intervals displays 12 h-like patterning, with the Cmax following closely after each application and the overall 24 h Cmin occurring during sleep (Figure 3A).
The Jatenzo® oral soft gel capsule formulation ingested twice daily at equal intervals also gives rise to variable TT levels of distinct 12 h patterning, with prominent Cmax following 2 to 4 h after each ingestion and rapidly declining levels thereafter (Figure 3B).
Xyosted®, a patient subcutaneously injected TRT at weekly intervals, has yet to be rigorously evaluated for its TT day-night pattern. Available data based upon rather infrequent blood sampling indicate Cmax occurs approximately 12 h following each weekly administration and that TT is maintained within the therapeutic range in a relatively stable manner, at least throughout the initial days of the 7-day dosing period (Figure 3C).
*The TT concentration produced by the Androderm® transdermal patch applied to the skin of the back, stomach, upper arms, or thighs nightly before retiring to sleep more closely reproduces the normative TT circadian pattern of young adult males than any of the other marketed PA-TRTs. Following application, TT concentration progressively rises during sleep and peaks around the time of morning awakening; it progressively declines during late morning and afternoon, reaching its nadir (Cmin) in the evening before the next scheduled patch application (Figure 3D).
I have been at this way too long!
troughs of natural T? - Excel Male TRT Forum
just curious folks who were borderline low T how much of a difference getting bloods an hour or 2 later in the day? ie are u 400 when woke up and bloods later in the day how much lower did they get? anyway, ive only seen charts of folks with normal T start at 700 and go down to 300 or so...

A pill that could outsell Viagra: New testosterone Rx drug - Excel Male TRT Forum
https://www.americanbazaaronline.com/2022/10/11/testosterone-drug-kyzatrex-hits-market-451261/ Kyzatrex could be a potential blockbuster to treat testosterone deficiency, a severely undertreated disease. Testosterone has been historically perceived as a lifestyle issue for men who want to...
Who Started TRT w/ "Normal" Levels @ What Age? - Page 3 - Excel Male TRT Forum
Latest labs in August were all middle range, slightly lower for my age. I turn 45 tomorrow and I feel fine, mostly, but 'things aren't what they used to be'. All my friends my age are on TRT, and some telling to do 150+ once a week. That seems extreme to me with my numbers...
Official Natesto Thread - Page 5 - Excel Male TRT Forum
Welcome to the Natesto thread. I have used Natesto on an off for several years, but it seems to be one of the less popular TRT options here. That said, I have seen a few readers mention it, and I thought it would be good to start a dedicated thread on Natesto where people can share their...
Gel or inject ? - Excel Male TRT Forum
I have been using T gel for many years, 2 packets of 1% , 50mg /packet / day. I am considering a change to injectable test/cyp, really just for the cost factor. I just moved to medicare and the deductable plus the cost of the gel is pretty high. I am wondering about the cycle of high to low...
Tips on how to blend propionate with enanthate (or cypionate)? - Page 4 - Excel Male TRT Forum
I have been having some success with low dose daily propionate for the last several months. Dose levels have ranged from 8-10 mg injected every morning after waking. Overall, it has been a far better experience than my previous cypionate protocol of 80-100 per week (split every 3.5 days)...

ANDRODERM® (TDS) - Excel Male TRT Forum
https://www.androderm.com/about-androderm ANDRODERM® (testosterone transdermal system) is designed to deliver testosterone continuously for 24 hours following application to intact, non-scrotal skin (e.g., back, abdomen, thighs, upper arms). Four strengths of ANDRODERM® are available that...
Water retention when I inject @ evening and less when @ morning, ideas why ? - Excel Male TRT Forum
I feel the best emotionally and get the best sleep as close to being natty when I inject ED around 12,5mg Test Prop in the evening prior to bed. Been experimenting for quite some time and indeed there is a very big difference. Wake up full of energy and feel calm during the day. Also this...
Best time to inject Test - Evening? - Excel Male TRT Forum
When is the best time of day to inject Test C or HCG? Natural testosterone is highest in the morning so it seems injecting Test in the evening is the best option? Don't have any idea when the best time to inject HCG is.
Still trying to find libido - Page 3 - Excel Male TRT Forum
I’ve been on topical cream (not applied to testicles) and now shots. I was on the 100mg dose of cream and that brought my dht up but not my t. So I switched to shots. I’ve been taking daily shots now for 6 weeks at 150mg per week. My shbg is 15, e2 47, t-778, ft- 159 (max is 155). It seems one...
New thoughts on AI - Excel Male TRT Forum
I was curious if you all have seen some of the latest research, and doctors on YouTube, other forums Etc. advocating to not block estradiol i.e. do not take an AI – and that it is more beneficial and causes no harm to let estrogen reach its own level when on testosterone supplementation. Have...
Applying cream twice a day problems - Excel Male TRT Forum
To those of you applying cream BID, do you have sleep issues after applying the second dose at night. Cream seems to be very activating and I can’t sleep at night when I apply the second dose. If I just apply the morning dose I sleep fine. Anybody else have this issue ?
Creams with new application over injectable? - Excel Male TRT Forum
Hi all - I've heard many problems with creams both here and from other sources. However, this recent Tweet from Dr. Jay Campbell got me curious: Has anyone heard about this? What do you think? They're doing 2x / day application which would theoretically lead to more stable levels...
Case Study: Absorption of Testosterone Cream via Scrotal Delivery
Case Study: Absorption of Testosterone Cream via Scrotal Delivery. Needham S1, Needham S2. 1Moses Lake Professional Pharmacy, Moses Lake, Washington. 2Alturas Analytics in Moscow, Idaho. Abstract Transdermal testosterone has been used for years to treat patients with low testosterone...
You possess an extraordinary amount of knowledge. If doctors knew even a fraction of what you know...If anything you are getting 2 daily peak/troughs 24/7.
T levels will be much lower before it is time for your second dose (12 hrs after 1st dose) let alone after you take your second dose you will hit a high Cmax 2-4 hrs later than T levels would rapidly decline and will be much lower overnight until your next dose in the early AM.
Even if dosed once daily which no one would do your T levels would be much lower in the evening/throughout the night until your next morning dose.
Many fail to realize that T levels gradually rise overnight reaching peak in the earl AM.
*elevated and near peak TT level during nighttime sleep, peak TT level around the time of morning awakening
*T production occurs in the greatest amount during sleep as recurring pulses at approximately 90 min intervals in healthy young males and approximately 140 min in healthy middle-aged males (91).
This is key:
(i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
*There are substantial differences between the therapies in the derived TT 24 h pattern; moreover, all but one of them differs either somewhat or greatly from the normative one of diurnally active young adult males, which is defined by:
(i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
*The serum TT concentration generated by the Striant® mucoadhesive buccal tablet system applied to the upper gum above the incisor of either side of the mouth twice daily at equal intervals displays 12 h-like patterning, with the Cmax following closely after each application and the overall 24 h Cmin occurring during sleep (Figure 3A).
*The Jatenzo® oral soft gel capsule formulation ingested twice daily at equal intervals also gives rise to variable TT levels of distinct 12 h patterning, with prominent Cmax following 2 to 4 h after each ingestion and rapidly declining levels thereafter (Figure 3B).
*As shown in the graphs of Figures 2 and 3, the PK of most FDA-approved PA-TRTs gives rise to TT 24 h patterns that deviate greatly from the normative one thereby failing to satisfy one or more of the five specified criteria.
*AndroGel® 1%, AndroGel® 1.62%, Xyosted®, and Striant®, which achieve relatively constant serum hormone concentration throughout the 24 h, seem to have been incorrectly conceptualized, perhaps because of the presumed necessity to maintain nonvarying, that is, homeostatic, TT concentration to achieve consistency of biological effects.
*The FDA-approved gel and solution PA-TRTs when applied as directed, that is, morning after awakening from nighttime sleep, while achieving TT levels within the normal range to remedy androgen hormone deficiency, fail to restore the normal physiologic TT circadian variation.
*The temporal patterns of these PA-TRTs differ from normal, either in the timing of the peak and/or nadir TT concentrations, by achieving the highest hormone levels generally between midmorning and noon and lowest (rather than near peak) ones during sleep (Figure 2A-2F).
Does Patient-Applied TRT Pose Risk for Blood Pressure Elevation? - Excel Male TRT Forum
Does Patient-Applied Testosterone Replacement Therapy Pose Risk for Blood Pressure Elevation? Circadian Medicine Perspectives (2022) Michael H. Smolensky, Ramon C. Hermida, Linda Sackett-Lundeen, *Ramon G. Hermida-Ayala, and Yong-Jian Geng ABSTRACT We reviewed medication package inserts, US...
*The US Food and Drug Administration (FDA), since the 1950s, has approved several physician-administered injectables and implantable pellets plus 10 unique (nonbiologically similar) patient-applied (PA) transdermal gel, intranasal gel, transdermal solutions, skin patches, buccal tablet, oral capsule, and subcutaneously injected TRTs. Intramuscularly injected and surgically implanted TRTs are administered by healthcare professionals at intervals of several weeks or months, whereas PA transdermal gel and solutions are dosed once daily at the commencement of the activity period, buccal tablet and oral soft gel capsule two times daily at approximately 12 h intervals, intranasal gel three-times daily at approximately 6 to 8 h intervals, and transdermal patch once daily before bedtime. As subsequently discussed, there is a substantial difference in the pharmacokinetics (PK) and attained T 24 h patterning between the 10 different PA-TRTs.
*LH pulses exhibit 24 h temporal patterning; they occur in greater number and higher amplitude during the sleep than wake span, suggesting the involvement of sleep-facilitating or sleep-dependent processes (10, 17, 57, 164, 175–177). Consequently, T production occurs in the greatest amount during sleep as recurring pulses at approximately 90 min intervals in healthy young males and approximately 140 min in healthy middle-aged males (91).
*Figures 2A-2F depict the TT 24 h pattern achieved by the 6 different solution and gel PA-TRTs, and Figures 3A-3D depict the TT 24 h pattern achieved by the buccal tablet, oral capsule, transdermal patch, and subcutaneously injected PATRTs. There are substantial differences between the therapies in the derived TT 24 h pattern; moreover, all but one of them differs either somewhat or greatly from the normative one of diurnally active young adult males, which is defined by: (i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
AndroGel® 1%, AndroGel® 1.62%, Axiron®, Fortesta®, and Testim® (and its biosimilar Vogelxo®) gel and solution preparations are recommended for application once daily in the morning to attain the highest serum hormone level 2 to 6 h following dosing and lowest, instead of highest, hormone level during sleep, that is, final hours of the 24 h dosing interval (Figure 2A-2E).
The Natesto® gel product applied to each nostril three times daily at approximately equal intervals results in highly variable serum TT concentration during the 24 h, showing three prominent peaks (Cmax), each occurring approximately 40 min after the administrations, and three prominent nadirs (Cmin) of 2 to 4 h duration, each occurring midway through the dosing intervals (Figure 2F).
The serum TT concentration generated by the Striant® mucoadhesive buccal tablet system applied to the upper gum above the incisor of either side of the mouth twice daily at equal intervals displays 12 h-like patterning, with the Cmax following closely after each application and the overall 24 h Cmin occurring during sleep (Figure 3A).
The Jatenzo® oral soft gel capsule formulation ingested twice daily at equal intervals also gives rise to variable TT levels of distinct 12 h patterning, with prominent Cmax following 2 to 4 h after each ingestion and rapidly declining levels thereafter (Figure 3B).
Xyosted®, a patient subcutaneously injected TRT at weekly intervals, has yet to be rigorously evaluated for its TT day-night pattern. Available data based upon rather infrequent blood sampling indicate Cmax occurs approximately 12 h following each weekly administration and that TT is maintained within the therapeutic range in a relatively stable manner, at least throughout the initial days of the 7-day dosing period (Figure 3C).
*The TT concentration produced by the Androderm® transdermal patch applied to the skin of the back, stomach, upper arms, or thighs nightly before retiring to sleep more closely reproduces the normative TT circadian pattern of young adult males than any of the other marketed PA-TRTs. Following application, TT concentration progressively rises during sleep and peaks around the time of morning awakening; it progressively declines during late morning and afternoon, reaching its nadir (Cmin) in the evening before the next scheduled patch application (Figure 3D).
I have been at this way too long!
troughs of natural T? - Excel Male TRT Forum
just curious folks who were borderline low T how much of a difference getting bloods an hour or 2 later in the day? ie are u 400 when woke up and bloods later in the day how much lower did they get? anyway, ive only seen charts of folks with normal T start at 700 and go down to 300 or so...
A pill that could outsell Viagra: New testosterone Rx drug - Excel Male TRT Forum
https://www.americanbazaaronline.com/2022/10/11/testosterone-drug-kyzatrex-hits-market-451261/ Kyzatrex could be a potential blockbuster to treat testosterone deficiency, a severely undertreated disease. Testosterone has been historically perceived as a lifestyle issue for men who want to...
Who Started TRT w/ "Normal" Levels @ What Age? - Page 3 - Excel Male TRT Forum
Latest labs in August were all middle range, slightly lower for my age. I turn 45 tomorrow and I feel fine, mostly, but 'things aren't what they used to be'. All my friends my age are on TRT, and some telling to do 150+ once a week. That seems extreme to me with my numbers...
Official Natesto Thread - Page 5 - Excel Male TRT Forum
Welcome to the Natesto thread. I have used Natesto on an off for several years, but it seems to be one of the less popular TRT options here. That said, I have seen a few readers mention it, and I thought it would be good to start a dedicated thread on Natesto where people can share their...
Gel or inject ? - Excel Male TRT Forum
I have been using T gel for many years, 2 packets of 1% , 50mg /packet / day. I am considering a change to injectable test/cyp, really just for the cost factor. I just moved to medicare and the deductable plus the cost of the gel is pretty high. I am wondering about the cycle of high to low...
Tips on how to blend propionate with enanthate (or cypionate)? - Page 4 - Excel Male TRT Forum
I have been having some success with low dose daily propionate for the last several months. Dose levels have ranged from 8-10 mg injected every morning after waking. Overall, it has been a far better experience than my previous cypionate protocol of 80-100 per week (split every 3.5 days)...
ANDRODERM® (TDS) - Excel Male TRT Forum
https://www.androderm.com/about-androderm ANDRODERM® (testosterone transdermal system) is designed to deliver testosterone continuously for 24 hours following application to intact, non-scrotal skin (e.g., back, abdomen, thighs, upper arms). Four strengths of ANDRODERM® are available that...
Water retention when I inject @ evening and less when @ morning, ideas why ? - Excel Male TRT Forum
I feel the best emotionally and get the best sleep as close to being natty when I inject ED around 12,5mg Test Prop in the evening prior to bed. Been experimenting for quite some time and indeed there is a very big difference. Wake up full of energy and feel calm during the day. Also this...
Best time to inject Test - Evening? - Excel Male TRT Forum
When is the best time of day to inject Test C or HCG? Natural testosterone is highest in the morning so it seems injecting Test in the evening is the best option? Don't have any idea when the best time to inject HCG is.
Still trying to find libido - Page 3 - Excel Male TRT Forum
I’ve been on topical cream (not applied to testicles) and now shots. I was on the 100mg dose of cream and that brought my dht up but not my t. So I switched to shots. I’ve been taking daily shots now for 6 weeks at 150mg per week. My shbg is 15, e2 47, t-778, ft- 159 (max is 155). It seems one...
New thoughts on AI - Excel Male TRT Forum
I was curious if you all have seen some of the latest research, and doctors on YouTube, other forums Etc. advocating to not block estradiol i.e. do not take an AI – and that it is more beneficial and causes no harm to let estrogen reach its own level when on testosterone supplementation. Have...
Applying cream twice a day problems - Excel Male TRT Forum
To those of you applying cream BID, do you have sleep issues after applying the second dose at night. Cream seems to be very activating and I can’t sleep at night when I apply the second dose. If I just apply the morning dose I sleep fine. Anybody else have this issue ?
Creams with new application over injectable? - Excel Male TRT Forum
Hi all - I've heard many problems with creams both here and from other sources. However, this recent Tweet from Dr. Jay Campbell got me curious: Has anyone heard about this? What do you think? They're doing 2x / day application which would theoretically lead to more stable levels...
Case Study: Absorption of Testosterone Cream via Scrotal Delivery
Case Study: Absorption of Testosterone Cream via Scrotal Delivery. Needham S1, Needham S2. 1Moses Lake Professional Pharmacy, Moses Lake, Washington. 2Alturas Analytics in Moscow, Idaho. Abstract Transdermal testosterone has been used for years to treat patients with low testosterone...
My day/night pattern is skewed. My 'peak', based on rise in libido and corresponding erection, occurs around 10 p.m. No nocturnal erections or morning wood. And it doesn't matter when I take my injection.(currently 34 mg EOD at 6 p.m.) This circadian change is due to bipolar illness, since my ability to naturally sleep has disappeared. I've needed medication to sleep for the past 18 years and that isn't even quality sleep.
A once a night erection would be fine if my wife and I slept together but bipolar and her ambivalence about sex put an end to that. She's now 16 months into rapidly progressing Alzheimer's, with me as her sole caregiver. And that's the story.
What is your TRT protocol, Madman?If anything you are getting 2 daily peak/troughs 24/7.
T levels will be much lower before it is time for your second dose (12 hrs after 1st dose) let alone after you take your second dose you will hit a high Cmax 2-4 hrs later than T levels would rapidly decline and will be much lower overnight until your next dose in the early AM.
Even if dosed once daily which no one would do your T levels would be much lower in the evening/throughout the night until your next morning dose.
Many fail to realize that T levels gradually rise overnight reaching peak in the earl AM.
*elevated and near peak TT level during nighttime sleep, peak TT level around the time of morning awakening
*T production occurs in the greatest amount during sleep as recurring pulses at approximately 90 min intervals in healthy young males and approximately 140 min in healthy middle-aged males (91).
This is key:
(i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
*There are substantial differences between the therapies in the derived TT 24 h pattern; moreover, all but one of them differs either somewhat or greatly from the normative one of diurnally active young adult males, which is defined by:
(i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
*The serum TT concentration generated by the Striant® mucoadhesive buccal tablet system applied to the upper gum above the incisor of either side of the mouth twice daily at equal intervals displays 12 h-like patterning, with the Cmax following closely after each application and the overall 24 h Cmin occurring during sleep (Figure 3A).
*The Jatenzo® oral soft gel capsule formulation ingested twice daily at equal intervals also gives rise to variable TT levels of distinct 12 h patterning, with prominent Cmax following 2 to 4 h after each ingestion and rapidly declining levels thereafter (Figure 3B).
*As shown in the graphs of Figures 2 and 3, the PK of most FDA-approved PA-TRTs gives rise to TT 24 h patterns that deviate greatly from the normative one thereby failing to satisfy one or more of the five specified criteria.
*AndroGel® 1%, AndroGel® 1.62%, Xyosted®, and Striant®, which achieve relatively constant serum hormone concentration throughout the 24 h, seem to have been incorrectly conceptualized, perhaps because of the presumed necessity to maintain nonvarying, that is, homeostatic, TT concentration to achieve consistency of biological effects.
*The FDA-approved gel and solution PA-TRTs when applied as directed, that is, morning after awakening from nighttime sleep, while achieving TT levels within the normal range to remedy androgen hormone deficiency, fail to restore the normal physiologic TT circadian variation.
*The temporal patterns of these PA-TRTs differ from normal, either in the timing of the peak and/or nadir TT concentrations, by achieving the highest hormone levels generally between midmorning and noon and lowest (rather than near peak) ones during sleep (Figure 2A-2F).
Does Patient-Applied TRT Pose Risk for Blood Pressure Elevation? - Excel Male TRT Forum
Does Patient-Applied Testosterone Replacement Therapy Pose Risk for Blood Pressure Elevation? Circadian Medicine Perspectives (2022) Michael H. Smolensky, Ramon C. Hermida, Linda Sackett-Lundeen, *Ramon G. Hermida-Ayala, and Yong-Jian Geng ABSTRACT We reviewed medication package inserts, US...
*The US Food and Drug Administration (FDA), since the 1950s, has approved several physician-administered injectables and implantable pellets plus 10 unique (nonbiologically similar) patient-applied (PA) transdermal gel, intranasal gel, transdermal solutions, skin patches, buccal tablet, oral capsule, and subcutaneously injected TRTs. Intramuscularly injected and surgically implanted TRTs are administered by healthcare professionals at intervals of several weeks or months, whereas PA transdermal gel and solutions are dosed once daily at the commencement of the activity period, buccal tablet and oral soft gel capsule two times daily at approximately 12 h intervals, intranasal gel three-times daily at approximately 6 to 8 h intervals, and transdermal patch once daily before bedtime. As subsequently discussed, there is a substantial difference in the pharmacokinetics (PK) and attained T 24 h patterning between the 10 different PA-TRTs.
*LH pulses exhibit 24 h temporal patterning; they occur in greater number and higher amplitude during the sleep than wake span, suggesting the involvement of sleep-facilitating or sleep-dependent processes (10, 17, 57, 164, 175–177). Consequently, T production occurs in the greatest amount during sleep as recurring pulses at approximately 90 min intervals in healthy young males and approximately 140 min in healthy middle-aged males (91).
*Figures 2A-2F depict the TT 24 h pattern achieved by the 6 different solution and gel PA-TRTs, and Figures 3A-3D depict the TT 24 h pattern achieved by the buccal tablet, oral capsule, transdermal patch, and subcutaneously injected PATRTs. There are substantial differences between the therapies in the derived TT 24 h pattern; moreover, all but one of them differs either somewhat or greatly from the normative one of diurnally active young adult males, which is defined by: (i) elevated and near peak TT level during nighttime sleep, (ii) peak TT level around the time of morning awakening, (iii) moderately elevated TT level during the initial hours of wakefulness, (iv) reduced TT level in the late afternoon, and (v) lowest TT level in the evening. Based upon these criteria, only the Androderm® transdermal patch (Figure 3D), when applied in the evening (∼22:00 h) as recommended, closely mimics the TT circadian rhythm of normal young adult males.
AndroGel® 1%, AndroGel® 1.62%, Axiron®, Fortesta®, and Testim® (and its biosimilar Vogelxo®) gel and solution preparations are recommended for application once daily in the morning to attain the highest serum hormone level 2 to 6 h following dosing and lowest, instead of highest, hormone level during sleep, that is, final hours of the 24 h dosing interval (Figure 2A-2E).
The Natesto® gel product applied to each nostril three times daily at approximately equal intervals results in highly variable serum TT concentration during the 24 h, showing three prominent peaks (Cmax), each occurring approximately 40 min after the administrations, and three prominent nadirs (Cmin) of 2 to 4 h duration, each occurring midway through the dosing intervals (Figure 2F).
The serum TT concentration generated by the Striant® mucoadhesive buccal tablet system applied to the upper gum above the incisor of either side of the mouth twice daily at equal intervals displays 12 h-like patterning, with the Cmax following closely after each application and the overall 24 h Cmin occurring during sleep (Figure 3A).
The Jatenzo® oral soft gel capsule formulation ingested twice daily at equal intervals also gives rise to variable TT levels of distinct 12 h patterning, with prominent Cmax following 2 to 4 h after each ingestion and rapidly declining levels thereafter (Figure 3B).
Xyosted®, a patient subcutaneously injected TRT at weekly intervals, has yet to be rigorously evaluated for its TT day-night pattern. Available data based upon rather infrequent blood sampling indicate Cmax occurs approximately 12 h following each weekly administration and that TT is maintained within the therapeutic range in a relatively stable manner, at least throughout the initial days of the 7-day dosing period (Figure 3C).
*The TT concentration produced by the Androderm® transdermal patch applied to the skin of the back, stomach, upper arms, or thighs nightly before retiring to sleep more closely reproduces the normative TT circadian pattern of young adult males than any of the other marketed PA-TRTs. Following application, TT concentration progressively rises during sleep and peaks around the time of morning awakening; it progressively declines during late morning and afternoon, reaching its nadir (Cmin) in the evening before the next scheduled patch application (Figure 3D).
I have been at this way too long!
troughs of natural T? - Excel Male TRT Forum
just curious folks who were borderline low T how much of a difference getting bloods an hour or 2 later in the day? ie are u 400 when woke up and bloods later in the day how much lower did they get? anyway, ive only seen charts of folks with normal T start at 700 and go down to 300 or so...
A pill that could outsell Viagra: New testosterone Rx drug - Excel Male TRT Forum
https://www.americanbazaaronline.com/2022/10/11/testosterone-drug-kyzatrex-hits-market-451261/ Kyzatrex could be a potential blockbuster to treat testosterone deficiency, a severely undertreated disease. Testosterone has been historically perceived as a lifestyle issue for men who want to...
Who Started TRT w/ "Normal" Levels @ What Age? - Page 3 - Excel Male TRT Forum
Latest labs in August were all middle range, slightly lower for my age. I turn 45 tomorrow and I feel fine, mostly, but 'things aren't what they used to be'. All my friends my age are on TRT, and some telling to do 150+ once a week. That seems extreme to me with my numbers...
Official Natesto Thread - Page 5 - Excel Male TRT Forum
Welcome to the Natesto thread. I have used Natesto on an off for several years, but it seems to be one of the less popular TRT options here. That said, I have seen a few readers mention it, and I thought it would be good to start a dedicated thread on Natesto where people can share their...
Gel or inject ? - Excel Male TRT Forum
I have been using T gel for many years, 2 packets of 1% , 50mg /packet / day. I am considering a change to injectable test/cyp, really just for the cost factor. I just moved to medicare and the deductable plus the cost of the gel is pretty high. I am wondering about the cycle of high to low...
Tips on how to blend propionate with enanthate (or cypionate)? - Page 4 - Excel Male TRT Forum
I have been having some success with low dose daily propionate for the last several months. Dose levels have ranged from 8-10 mg injected every morning after waking. Overall, it has been a far better experience than my previous cypionate protocol of 80-100 per week (split every 3.5 days)...
ANDRODERM® (TDS) - Excel Male TRT Forum
https://www.androderm.com/about-androderm ANDRODERM® (testosterone transdermal system) is designed to deliver testosterone continuously for 24 hours following application to intact, non-scrotal skin (e.g., back, abdomen, thighs, upper arms). Four strengths of ANDRODERM® are available that...
Water retention when I inject @ evening and less when @ morning, ideas why ? - Excel Male TRT Forum
I feel the best emotionally and get the best sleep as close to being natty when I inject ED around 12,5mg Test Prop in the evening prior to bed. Been experimenting for quite some time and indeed there is a very big difference. Wake up full of energy and feel calm during the day. Also this...
Best time to inject Test - Evening? - Excel Male TRT Forum
When is the best time of day to inject Test C or HCG? Natural testosterone is highest in the morning so it seems injecting Test in the evening is the best option? Don't have any idea when the best time to inject HCG is.
Still trying to find libido - Page 3 - Excel Male TRT Forum
I’ve been on topical cream (not applied to testicles) and now shots. I was on the 100mg dose of cream and that brought my dht up but not my t. So I switched to shots. I’ve been taking daily shots now for 6 weeks at 150mg per week. My shbg is 15, e2 47, t-778, ft- 159 (max is 155). It seems one...
New thoughts on AI - Excel Male TRT Forum
I was curious if you all have seen some of the latest research, and doctors on YouTube, other forums Etc. advocating to not block estradiol i.e. do not take an AI – and that it is more beneficial and causes no harm to let estrogen reach its own level when on testosterone supplementation. Have...
Applying cream twice a day problems - Excel Male TRT Forum
To those of you applying cream BID, do you have sleep issues after applying the second dose at night. Cream seems to be very activating and I can’t sleep at night when I apply the second dose. If I just apply the morning dose I sleep fine. Anybody else have this issue ?
Creams with new application over injectable? - Excel Male TRT Forum
Hi all - I've heard many problems with creams both here and from other sources. However, this recent Tweet from Dr. Jay Campbell got me curious: Has anyone heard about this? What do you think? They're doing 2x / day application which would theoretically lead to more stable levels...
Case Study: Absorption of Testosterone Cream via Scrotal Delivery
Case Study: Absorption of Testosterone Cream via Scrotal Delivery. Needham S1, Needham S2. 1Moses Lake Professional Pharmacy, Moses Lake, Washington. 2Alturas Analytics in Moscow, Idaho. Abstract Transdermal testosterone has been used for years to treat patients with low testosterone...
I’ve been on TRT for about 7 years. No regrets.
I’ve tried enanthate, cypionate, cream, and propionate and like them in roughly that order. Tried just about every injection protocol too, eventually settling on EOD enanthate.
If I have any complaints, it’s that I’m jealous of the guys that benefit from low doses and normal levels. I find that I don’t get much benefit from TRT until my levels are in the upper part of the range or higher, and what goes with that are side effects like poor sleep and some acne.
Be aware that if you choose to try it, you will likely feel fantastic for a few days immediately upon starting. That is a dopamine response and is not indicative of how you’ll feel on TRT long term.
Also know that there is very little risk in trying it out. So many guys think that if you try it, you’re “stuck on it for life”. Using sensible doses, you could try it out for a few months then very likely go right back to your natural levels if you decide it’s not for you.
I’ve tried enanthate, cypionate, cream, and propionate and like them in roughly that order. Tried just about every injection protocol too, eventually settling on EOD enanthate.
If I have any complaints, it’s that I’m jealous of the guys that benefit from low doses and normal levels. I find that I don’t get much benefit from TRT until my levels are in the upper part of the range or higher, and what goes with that are side effects like poor sleep and some acne.
Be aware that if you choose to try it, you will likely feel fantastic for a few days immediately upon starting. That is a dopamine response and is not indicative of how you’ll feel on TRT long term.
Also know that there is very little risk in trying it out. So many guys think that if you try it, you’re “stuck on it for life”. Using sensible doses, you could try it out for a few months then very likely go right back to your natural levels if you decide it’s not for you.
Certainly give it a try! If it doesn’t work for you then stop and you will quickly go back to baseline. I’ve been on TRT for about 10 years, and following this forum 3 years. One factor to consider when reading other people’s experiences here is that many of them are taking way more T than what is considered normal. When it comes to T I found that more is not better! More does not give you more libido, but it will give you elevated red blood cell counts, acne,and a short temper. The only positive is more muscle mass and definition, but in my opinion that’s not worth the long list of negative side effects. I inject 40 mg twice a week and all systems are go. I added HCG a few months ago to see if my testicles would come back, and that worked. The hcg may have also presented an uptick in my libido, which was already very good. So try TRT, but go in baby steps, and do regular labs. You don’t need total T of 1500+ when everything works better at 750.
tropicaldaze1950
Well-Known Member
How much EOD?I’ve been on TRT for about 7 years. No regrets.
I’ve tried enanthate, cypionate, cream, and propionate and like them in roughly that order. Tried just about every injection protocol too, eventually settling on EOD enanthate.
If I have any complaints, it’s that I’m jealous of the guys that benefit from low doses and normal levels. I find that I don’t get much benefit from TRT until my levels are in the upper part of the range or higher, and what goes with that are side effects like poor sleep and some acne.
Be aware that if you choose to try it, you will likely feel fantastic for a few days immediately upon starting. That is a dopamine response and is not indicative of how you’ll feel on TRT long term.
Also know that there is very little risk in trying it out. So many guys think that if you try it, you’re “stuck on it for life”. Using sensible doses, you could try it out for a few months then very likely go right back to your natural levels if you decide it’s not for you.

36mg (126mg/wk)How much EOD?
Similar threads
- Replies
- 20
- Views
- 3K
- Replies
- 61
- Views
- 8K
- Replies
- 0
- Views
- 38
- Replies
- 28
- Views
- 4K
- Replies
- 31
- Views
- 2K


Sponsors








Online statistics
- Members online
- 8
- Guests online
- 225
- Total visitors
- 233
Totals may include hidden visitors.
Latest posts
-
-
 Ran out of wife's testosterone-can she use mine?
Ran out of wife's testosterone-can she use mine?- Latest: FunkOdyssey
-
-
TRT plus Low dose Ligandrol LGD-4033
- Latest: GreenMachineX
-
 The Gut Microbiome and Testosterone: An Intriguing Connection
The Gut Microbiome and Testosterone: An Intriguing Connection- Latest: Nelson Vergel
-
