Yes. It's very impressive with state-of-the-art pharmaceutical equipment. Over 115,000 sq feet in addition to the 50K square feet of the old building.
Where is it located?


Yes. It's very impressive with state-of-the-art pharmaceutical equipment. Over 115,000 sq feet in addition to the 50K square feet of the old building.

Are we talking years, do you think?Yes, they did. It will take a while to get a BLA approved.
7601 North Sam Houston Pkwy W #100, Houston, TX 77064Where is it located?
I am not sure. I would not be surprised if it takes two years.Are we talking years, do you think?
We are a 503B compounding pharmacy located in Oklahoma and have been manufacturing hormone pellets for years. Recently began production of Testosterone Cypionate 200 mg/ml available in 2 ml or 10 ml vials. We CANNOT make HCG due to being restricted by the FDA and anyone that does so without a Biologics license is doing to illegally.Couldn’t compounding pharmacies like Empower purchase brand name drugs like Testosterone, HCG, anastrozole etc and resell them at a mark up? So that TRT clinics could continue to send prescriptions to these compounding pharmacies. I know this doesn’t fix the problem of affordability and lack of treatment options for some people (specially women) but at least fix some of the accessibility issues.
The focus remains to avoid this to happen but just thinking about a plan B in case worst case scenario happens.
Updated June 07, 2021
Bulk Drug Substances Nominated for Use in Compounding Under Section 503B of the Federal Food, Drug, and Cosmetic Act
503B Category 1: Bulk Drug Substances Under Evaluation (see pdf)
** Designates bulk drug substances that are components of FDA approved drugs
• Anastrazole**
• DHEA (dehydroepiandrosterone) **
• Estradiol Cypionate**
• Estradiol**
• Estriol
• Estrone**
• Finasteride**
• Minoxidil**
• Nandrolone Decanoate**
• Progesterone**
• Testosterone**
• Testosterone Cypionate**
• Testosterone Propionate**
• Tretinoin**
Updated November 2, 2021
Bulk Drug Substances Nominated for Use in Compounding Under Section 503A of the Federal Food, Drug, and Cosmetic Act
Notice of Updates to Section 503A Categories
Additions to category 1
o Ammonium Tetrathiomolybdate – This bulk drug substance was nominated with sufficient supporting information to permit FDA to evaluate it and may be eligible for inclusion on the 503A Bulks List
o Enclomiphene Citrate- This bulk drug substance was nominated with sufficient supporting information to permit FDA to evaluate it and may be eligible for inclusion on the 503A Bulks List
503A Category 1 – Bulk Drug Substances Under Evaluation (see pdf)
• 7 Keto Dehydroepiandrosterone
• Enclomiphene Citrate
• L-Citrulline
• Melatonin
• Pregnenolone
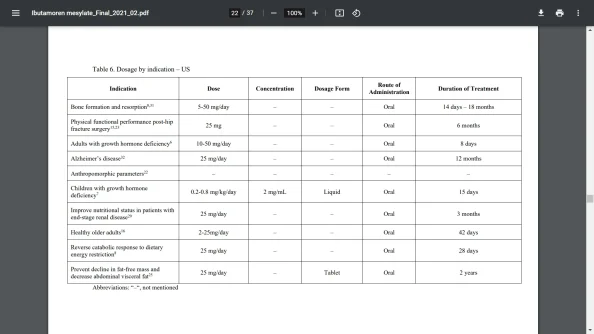
I wonder how they determined that ibutamoren has significant health risks. It is now approved for pediatric use in kids with growth retardation who need a GH stimulation test.

| Category 2 substance | Nominated with sufficient information under 503A or 503B or both | Date added to Category 2 | Safety risks |
|---|
.png")

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
Excellent summary. What do you think happens once all these go to Cat 2?I wondered what the impact of being categorized in one of these categories is, so I looked up the regulations. The net of it is as follows:
Category 1: Not on the approved list, but the FDA won't take any enforcement actions if they are compounded. FDA is evaluating and may one day add to the approved list.
Category 2 & 3: Cannot be compounded, unless it is an FDA approved drug and is on the FDA drug shortage list.
This is effectively a ban on ibutamoren from compounding pharmacies. Doesn't look like there is any end in sight for the FDA's war against compounding pharmacies. I guess they figure it's better for everybody to get things from the black market rather than being under the care of a physician and a well run pharmacy.











We use essential cookies to make this site work, and optional cookies to enhance your experience.