madman
Super Moderator
Background and Objective
In contemporary Urology, the gold standard for treatment of erectile dysfunction refractory to medical therapy has been implantation with a penile prosthesis. The past 40 years have witnessed evolutions in technology and surgical techniques, which have led to increased patient satisfaction rates and decreased complication and infection rates. This review is an update to a prior review article that evaluates these advancements in the context of patient satisfaction and different rates of complications following surgeries. In addition, the review compares malleable and inflatable prostheses with regard to infection rate, mechanical failure rate, and erosion rate.
Methods
A literature search was conducted using Medline and Google Scholar to examine papers from 1973 to the present day. Keywords, such as, “penile prosthesis surgery”, “malleable penile prosthesis”, “inflatable penile prosthesis”, “two-piece Inflatable Penile Prosthesis (IPP)”, and “three-piece IPP” were utilized during the search. A total of 76 papers were included, and all were in English.Key
Content and Findings
Studies on the latest models of each of the three prostheses (malleable, two-piece IPP, three-piece IPP) revealed patient satisfaction ratings at or above 75%. Both types of IPPs were associated with greater satisfaction and lower erosion rates while malleable prostheses were associated with lower mechanical failure rates. Although no significant differences in infection rates were noted between the prosthesis types, a history of diabetes, obesity, and smoking were predictive of infection events.
Conclusions
The three-piece IPP, if indicated for a suitable patient, is generally accepted as the best type of prosthesis given its biological mimicry to an erect human penis.
Introduction
In 1936, a Russian surgeon named Nikolaj Bogaraz designed the first autologous penile implant using a patient’s rib cartilage (1). A few decades later, the first inflatable penile prosthesis (IPP) and the Small-carrion malleable prosthesis were introduced in 1973 (2). In contemporary times, penile prostheses are the mainstay treatment for male urologic conditions, namely erectile dysfunction (ED) that is refractory to pharmacologic therapy. Penile prostheses are often classified as malleable (also known as semi-rigid), two-piece inflatable, or three-piece inflatable; each necessitating a distinct surgical technique. Of the three classes, the three-piece IPP is considered the most technologically advanced implant in the realm of penile prostheses and is used in the majority of penile implant surgeries (3). Prior reviewsof penile prostheses has stratified findings based on the type of prosthesis (i.e., two-piece) but not by the model type (i.e., Coloplast Titan). The present review is an update to our previously published article and emphasizes the postoperative outcomes of penile prosthesis procedures by implant type and model (4). We present this article in accordance with the Narrative Review reporting checklist (available at Recent technological development of penile prosthesis: a literature review - Patel- Translational Andrology and Urology).
Malleable prostheses
Historical perspective
Technological development of malleable prostheses
New Tactra, Rigi10, and touchless memory shape prostheses
Surgical considerations and post-operative results for malleable implants
Inflatable prostheses
Two-piece IPP
Historical perspective
Technological development of two-piece prostheses
Surgical Considerations and post-operative results for Two-piece Implants
Three-piece inflatable prostheses
Historical perspective
Technological development of 3-piece prostheses
Cylinder development
Antibacterial coatings
Pump development
Reservoir development
Latest 3-piece IPP developments
Surgical considerations and post-operative results for3-piece implants
Cylinders
Infection control
Reservoirs
*Predictive factors and comparison of IPP and malleable prostheses in infection rates, erosion rates, and mechanical dysfunction
Conclusions
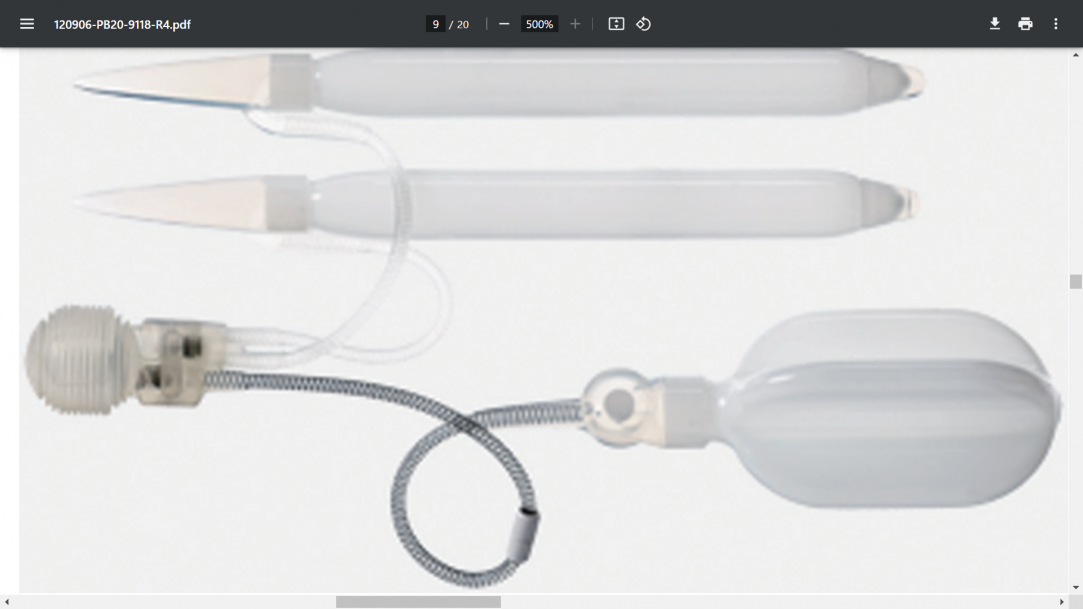
Since the early 1980s, advancements in technology and surgical techniques have transformed penile prosthetic implants. The unique features of various models of the three types of implants from this review paper are summarized in Table 6 with associated images (114-122). The use of advanced polymeric prosthetic materials, antibiotic coatings, and increased length and width options have led to improvements in functionality, strength, and device longevity. Concurrently, these advances have also decreased both infections and overall complication rates (123). Studies on the latest models of the three penile prosthetic device types reveal patient satisfaction ratings consistently at or above 75% (42,43,45,110-112). Two- and three-piece IPPs were associated with greater satisfaction, lower erosion rates, and higher failure mechanical rates compared to malleable prostheses. No notable differences in infection rate were found between IPPs and malleable prostheses, though diabetes, obesity, and a history of smoking were associated with higher infection rates. Given that a patient is a suitable candidate for a 3-piece IPP, many experts consider this device type to be the highest standard for biological mimicry of an erect human penis.
In contemporary Urology, the gold standard for treatment of erectile dysfunction refractory to medical therapy has been implantation with a penile prosthesis. The past 40 years have witnessed evolutions in technology and surgical techniques, which have led to increased patient satisfaction rates and decreased complication and infection rates. This review is an update to a prior review article that evaluates these advancements in the context of patient satisfaction and different rates of complications following surgeries. In addition, the review compares malleable and inflatable prostheses with regard to infection rate, mechanical failure rate, and erosion rate.
Methods
A literature search was conducted using Medline and Google Scholar to examine papers from 1973 to the present day. Keywords, such as, “penile prosthesis surgery”, “malleable penile prosthesis”, “inflatable penile prosthesis”, “two-piece Inflatable Penile Prosthesis (IPP)”, and “three-piece IPP” were utilized during the search. A total of 76 papers were included, and all were in English.Key
Content and Findings
Studies on the latest models of each of the three prostheses (malleable, two-piece IPP, three-piece IPP) revealed patient satisfaction ratings at or above 75%. Both types of IPPs were associated with greater satisfaction and lower erosion rates while malleable prostheses were associated with lower mechanical failure rates. Although no significant differences in infection rates were noted between the prosthesis types, a history of diabetes, obesity, and smoking were predictive of infection events.
Conclusions
The three-piece IPP, if indicated for a suitable patient, is generally accepted as the best type of prosthesis given its biological mimicry to an erect human penis.
Introduction
In 1936, a Russian surgeon named Nikolaj Bogaraz designed the first autologous penile implant using a patient’s rib cartilage (1). A few decades later, the first inflatable penile prosthesis (IPP) and the Small-carrion malleable prosthesis were introduced in 1973 (2). In contemporary times, penile prostheses are the mainstay treatment for male urologic conditions, namely erectile dysfunction (ED) that is refractory to pharmacologic therapy. Penile prostheses are often classified as malleable (also known as semi-rigid), two-piece inflatable, or three-piece inflatable; each necessitating a distinct surgical technique. Of the three classes, the three-piece IPP is considered the most technologically advanced implant in the realm of penile prostheses and is used in the majority of penile implant surgeries (3). Prior reviewsof penile prostheses has stratified findings based on the type of prosthesis (i.e., two-piece) but not by the model type (i.e., Coloplast Titan). The present review is an update to our previously published article and emphasizes the postoperative outcomes of penile prosthesis procedures by implant type and model (4). We present this article in accordance with the Narrative Review reporting checklist (available at Recent technological development of penile prosthesis: a literature review - Patel- Translational Andrology and Urology).
Malleable prostheses
Historical perspective
Technological development of malleable prostheses
New Tactra, Rigi10, and touchless memory shape prostheses
Surgical considerations and post-operative results for malleable implants
Inflatable prostheses
Two-piece IPP
Historical perspective
Technological development of two-piece prostheses
Surgical Considerations and post-operative results for Two-piece Implants
Three-piece inflatable prostheses
Historical perspective
Technological development of 3-piece prostheses
Cylinder development
Antibacterial coatings
Pump development
Reservoir development
Latest 3-piece IPP developments
Surgical considerations and post-operative results for3-piece implants
Cylinders
Infection control
Reservoirs
*Predictive factors and comparison of IPP and malleable prostheses in infection rates, erosion rates, and mechanical dysfunction
Conclusions
Since the early 1980s, advancements in technology and surgical techniques have transformed penile prosthetic implants. The unique features of various models of the three types of implants from this review paper are summarized in Table 6 with associated images (114-122). The use of advanced polymeric prosthetic materials, antibiotic coatings, and increased length and width options have led to improvements in functionality, strength, and device longevity. Concurrently, these advances have also decreased both infections and overall complication rates (123). Studies on the latest models of the three penile prosthetic device types reveal patient satisfaction ratings consistently at or above 75% (42,43,45,110-112). Two- and three-piece IPPs were associated with greater satisfaction, lower erosion rates, and higher failure mechanical rates compared to malleable prostheses. No notable differences in infection rate were found between IPPs and malleable prostheses, though diabetes, obesity, and a history of smoking were associated with higher infection rates. Given that a patient is a suitable candidate for a 3-piece IPP, many experts consider this device type to be the highest standard for biological mimicry of an erect human penis.