Hi there,
I'd really appreciate any thoughts or guidance on protocol/results below. I am quite surprised by the prolactin result, and even the T and E result as I am on a low daily dose and this is before my next injection. Any thoughts would be very appreciated. Purpose is TRT and not sport.
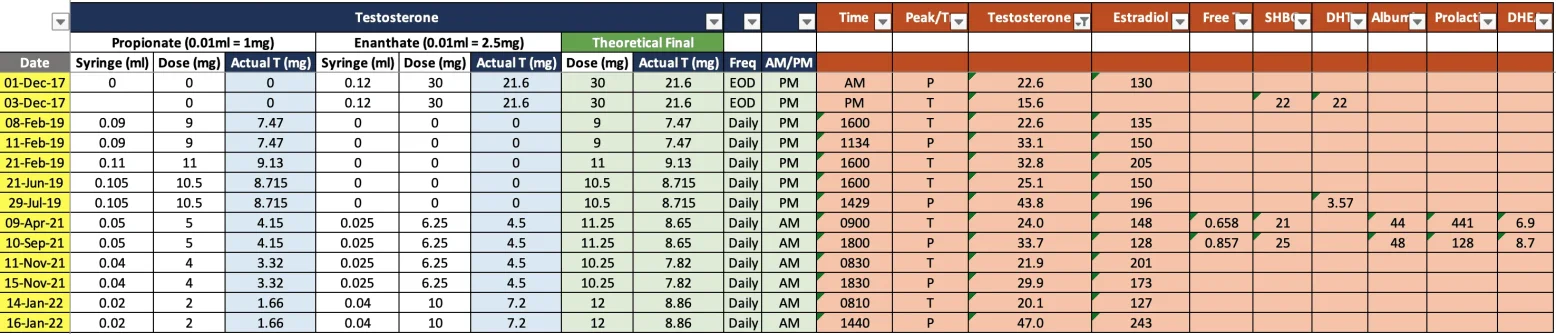
Protocol
Frequency: Daily subq injections
Enanthate: 6.25mg
Propionate: 5mg
Total T in syringe: 11.25mg (translates to 8.65mg daily Testosterone when you remove weight of ester)
HCG: None
AI: None
Injection site: subq in midsection
Time: 9am every morning
Result - 08:30am ('before' daily injection)
Albumin 44 g/L (Range: 34 - 50)
SHBG 21 nmol/L (Range: 16 - 55)
FSH 0.3 IU/L (Range: 1.5 - 12.4)
LH 0.5 IU/L (Range: 1.7 - 8.6)
Oestradiol 148 pmol/L (Range: < 192)
Testosterone 24.0 nmol/L (Range: 7.6 - 31.4)
Free Testosterone - Calc. 0.658 nmol/L (Range: 0.2 - 0.62)
Free Androgen Index 114.3 (Range: 24 - 104)
Prolactin 441 mIU/L (Range: 86 - 324)
DHEA Sulphate 6.9 umol/L (Range: 0.44 - 13.4)
Questions
1. Is my prolactin extremely high? Should I be worried? What could the causes be?
2. Is this my theoretical trough value as test was taken before my next injection? I'm not sure if there are other systems in the body (e.g. during sleep) that may elevate the result taken at 0830. Is it likely I'd have a lower result in the earlier hours?
3. Assuming that this is my trough value, it is expected that I will hit my peak value after the daily injection. Given my protocol, when is the peak expected to occur? After 4-6 hours? I am expecting a much higher result. I have not yet taken this blood test reading as I want to fix the trough first.
4. My blood test last year where the protocol was more or less the same - no Enanthate, only Propionate at higher dose. I had higher T and E values but much lower Prolactin values. Can someone explain how this would make sense?
Thanks,
R2
I'd really appreciate any thoughts or guidance on protocol/results below. I am quite surprised by the prolactin result, and even the T and E result as I am on a low daily dose and this is before my next injection. Any thoughts would be very appreciated. Purpose is TRT and not sport.
Protocol
Frequency: Daily subq injections
Enanthate: 6.25mg
Propionate: 5mg
Total T in syringe: 11.25mg (translates to 8.65mg daily Testosterone when you remove weight of ester)
HCG: None
AI: None
Injection site: subq in midsection
Time: 9am every morning
Result - 08:30am ('before' daily injection)
Albumin 44 g/L (Range: 34 - 50)
SHBG 21 nmol/L (Range: 16 - 55)
FSH 0.3 IU/L (Range: 1.5 - 12.4)
LH 0.5 IU/L (Range: 1.7 - 8.6)
Oestradiol 148 pmol/L (Range: < 192)
Testosterone 24.0 nmol/L (Range: 7.6 - 31.4)
Free Testosterone - Calc. 0.658 nmol/L (Range: 0.2 - 0.62)
Free Androgen Index 114.3 (Range: 24 - 104)
Prolactin 441 mIU/L (Range: 86 - 324)
DHEA Sulphate 6.9 umol/L (Range: 0.44 - 13.4)
Questions
1. Is my prolactin extremely high? Should I be worried? What could the causes be?
2. Is this my theoretical trough value as test was taken before my next injection? I'm not sure if there are other systems in the body (e.g. during sleep) that may elevate the result taken at 0830. Is it likely I'd have a lower result in the earlier hours?
3. Assuming that this is my trough value, it is expected that I will hit my peak value after the daily injection. Given my protocol, when is the peak expected to occur? After 4-6 hours? I am expecting a much higher result. I have not yet taken this blood test reading as I want to fix the trough first.
4. My blood test last year where the protocol was more or less the same - no Enanthate, only Propionate at higher dose. I had higher T and E values but much lower Prolactin values. Can someone explain how this would make sense?
Thanks,
R2