Can you post pic of the results? I could not open the spreadsheet. Also, are you subq or IM?Hi @Cataceous, @Willyt,
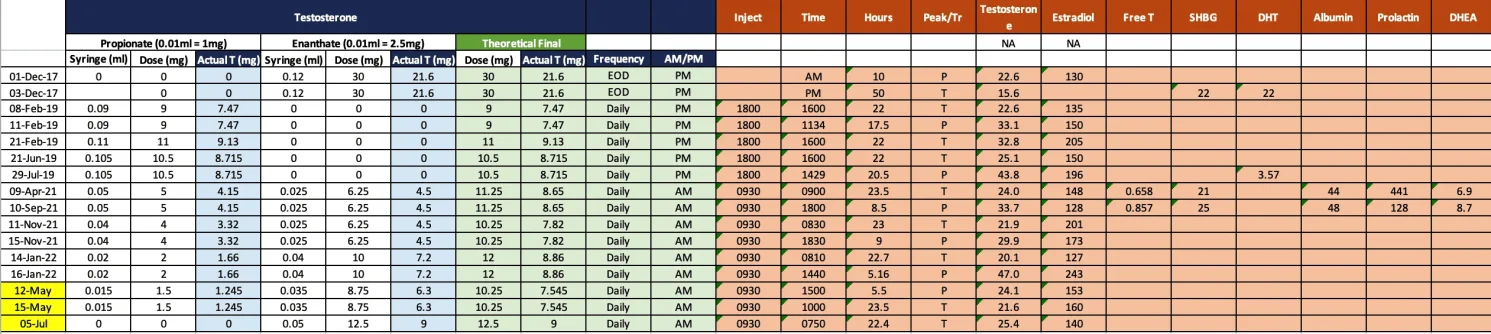
By way of an update, please see my results since February attached.
I think my Peak result in May is incorrect - I think I missed the Propionate peak, somewhat evident by the higher estradiol value in the Trough result.
In terms of my most recent July result, this is on the Enanthate only protocol of 12.5mg / 9mg (actual T) per day. I tested only the Trough/AM result on the basis that there is very little variation on such a protocol.
@Cataceous, would you suggest that I test a PM / theoretical peak result on the Enanthate only protocol anyway? Any thoughts on the result (T: 25.4 nmol/L, E:140 pmol/L)? I'm not sure where to go from here e.g. reduce the dose? Reduce and combine with Gel to increase variation? (I'm not keen on introducing the Propionate due to its disproportional effect and the potential uncontrolled/questionable source)
Subjective results on the Enan only protocol:
++
- More controllable acne (although still present)
- Less erratic mood (On the Prop/Enan blend, I became quite morbid/pessimistic each evening)
--
- Much reduced erectile quality; much softer and less lasting
- Increased anxiety in social situations when I am presenting to senior folks at work
- Less zest/interest for outdoor activities e.g. on the Prop/Enan blend, I was partaking in outdoor hobbies much more than now
- Sleep quality is worse
Thoughts appreciated on how I ought to amend my protocol to increase variation before I dive into new changes. Many thanks
Sounds like you're still on high side. Have you tried lowering to the much heralded 10mg Enan? (7.2 actual T per day). This seems to be sweet spot for many and is in line with average daily levels of healthy male.
On the sleep front, this is one area where prop/enan blend shines. You peak during day and let levels drop overnight. I sleep so much better on the blend.