The testing method used.
The most accurate assays for TT/estradiol/DHT (LC/MS-MS) and FT (Equilibrium Dialysis or Ultrafiltration).
Critical to have your FT tested using what would be considered the most accurate assays (Equilibrium Dialysis or Ultrafiltration), especially in cases of altered SHBG.
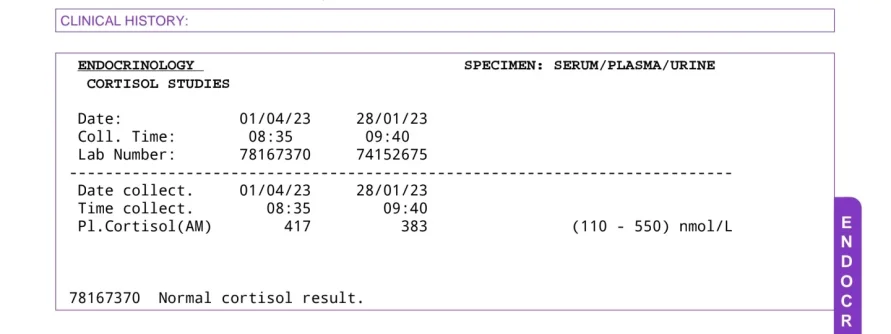
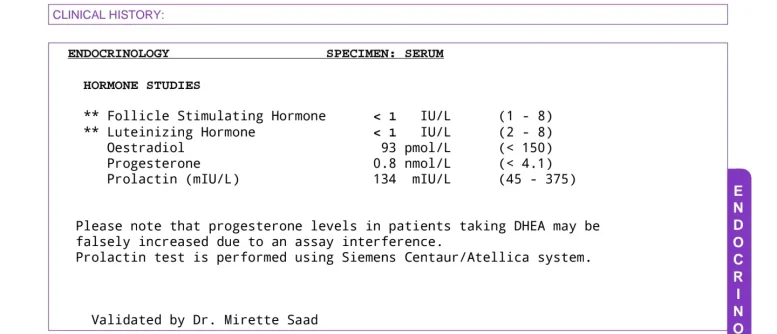
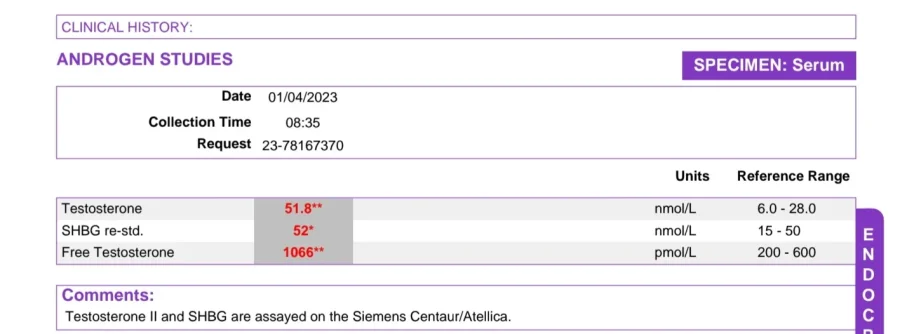
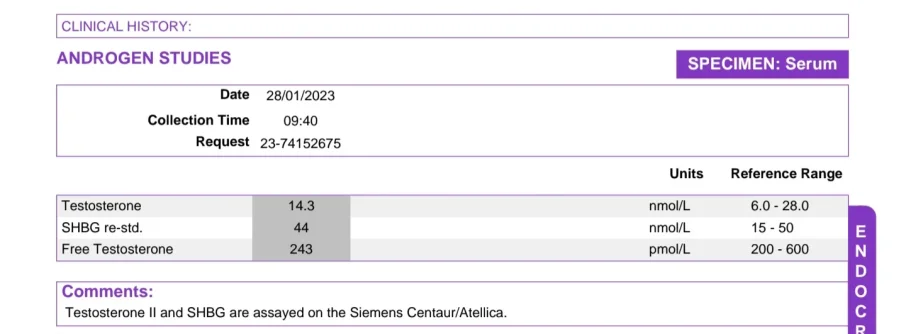
Your TT, SHBG, and estradiol were done using the direct immunoassay and FT was most likely calculated.
Look over the threads in post #6 when you have time!
https://www.hormoneassays.org/ Watch our video to learn about the importance of accurate hormone testing. Tests to measure the level of a specific hormone in the body are the third most common diagnostic in medicine today yet some current hormone tests are not sufficiently accurate or...

www.excelmale.com
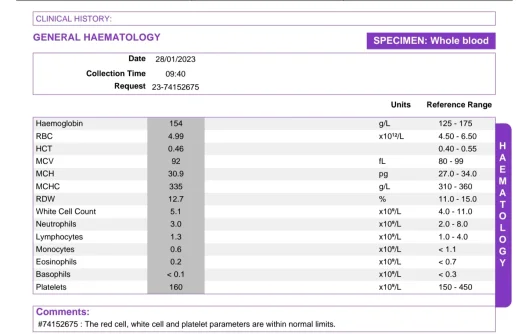
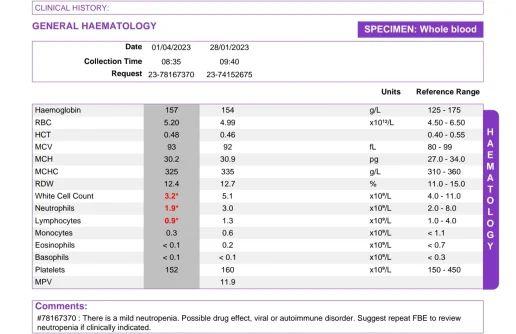
You are missing lab work for CBC which will include critical blood markers RBCs, hemoglobin, and hematocrit.
Post up your numbers as these are critical to know at the 6-week mark after starting TRT.
Would be interesting to see where your DHT sits on your current protocol.
Also, post up your pre-TRT labs.
Keep in mind that when first starting TRT or tweaking a protocol (dose/injection frequency) hormones will be in flux during the weeks leading up until blood levels have stabilized (4-6 weeks TC/TE) and it is common to experience ups/downs during the transition as the body is trying to adjust.
Mind you most will experience what we call the honeymoon period euphoric-like state, a strong increase in libido, spontaneous/nocturnal/morning erections due to increased dopamine/T levels rising/AR lighting up.
Unfortunately, this is short-lived and temporary as the body will adjust and eventually level out.
Keep in mind that once blood levels have stabilized it will take time for the body to adapt to the new set-point and this is the critical time period when one should gauge how they truly feel overall regarding relief/improvement of low-t symptoms.
The first 4-6 weeks can be very misleading when looking at the bigger picture.
Every protocol should be given 12 weeks before claiming it was a success or failure.
Always best to start low and go slow on a T-only protocol as we want to see how our body reacts to testosterone.
Lab work is done at the 6-week mark as we want to see where our trough TT, FT, estradiol, SHBG, and other important blood markers such as RBCs, hemoglobin, and hematocrit sit.
The only time the T dose should be increased at the 6-week mark is if your trough level is still too low (highly unlikely in most cases) which would result in a lack of improvement in low T symptoms.
On the other extreme many men are started on a high-dose protocol off the hop and end up struggling with sides/feeling unwell 6 weeks in because they are running too high a trough FT.
Too low or too high FT can easily have a negative impact on energy, mood, libido, and erectile function.
You can try and tough it out a little longer before deciding on your next move.
Only time will tell.
Even then you may fair better running a lower trough FT level.
You can look into adding low dose hCG eventually but keep in mind that it will drive up your TT, FT, and estradiol so you would need to make sure that you lower your T dose enough.
Would be a bad move to up your dose!



") appreciate your knowledgeable
appreciate your knowledgeable