

Nelson Vergel
Founder, ExcelMale.com

ExcelMale.com Quick Guide:
Diagnosis and Management of Hypogonadism
DIAGNOSIS OF HYPOGONADISM:
Symptoms and signs suggestive of testosterone deficiency in men:
A. More specific symptoms and signs
• Incomplete or delayed sexual development, eunuchoidism
• Reduced sexual desire (libido) and activity
• Decreased spontaneous erections during sleep
• Breast discomfort, gynecomastia
• Loss of body (axillary and pubic) hair, reduced shaving
• Very small (especially <5 ml) or shrinking testes
• Inability to father children, low or zero sperm count
• Height loss, low trauma fracture, low bone mineral density
• Hot flashes, sweats
B. Other less specific symptoms and signs
• Decreased energy, motivation, initiative, and self-confidence
• Feeling sad or blue, depressed mood, dysthymia
• Poor concentration and memory
· Decreased penile sensitivity
• Sleep disturbance, increased sleepiness
• Mild anemia (normochromic, normocytic, in the female range)
• Reduced muscle bulk and strength
• Increased body fat, body mass index
• Diminished physical or work performance
ADAM questionnaire about symptoms of low testosterone
(Androgen Deficiency in the Aging Male)
This basic questionnaire can be very useful for men to describe the kind and severity of their low testosterone symptoms.
1. Do you have a decrease in libido (sex drive)? Yes No
2. Do you have a lack of energy? Yes No
3. Do you have a decrease in strength and/or endurance? Yes No
4. Have you lost height? Yes No
5. Have you noticed a decreased “enjoyment of life” Yes No
6. Are you sad and/or grumpy? Yes No
7. Are your erections less strong? Yes No
8. Have you noticed a recent deterioration in your ability to play sports? Yes No
9. Are you falling asleep after dinner? Yes No
10. Has there been a recent deterioration in your work performance? Yes No
If patient answers Yes to number 1 or 7 or if he answers Yes to more than 3 questions, he may have hypogonadism.
Blood Tests and Physical Exam:
Total testosterone (TT) blood level of 400 ng/dL or below along with hypogonadism symptoms not caused by temporary factors (lack of sleep, recent excess weight gain, thyroid dysfunction, temporary illness, and anabolic steroid use). For men with TT > 400 ng/dL, lifestyle modification counseling to lower BMI (If BMI >26), improve sleep hygiene, and exercise is recommended. These are other interventions that may increase testosterone in men: How to Increase Testosterone Naturally
Free Testosterone (FT) blood levels should be at least 2 percent of TT. Not much can be done to manipulate sex hormone binding globulin (SHBG) to increase FT levels since it may be determined by genetics, comorbidities, insulin or inflammation. People with diabetes and hyperglycemia may have lower levels of sex hormone binding globulin even in the presence of low TT. Men on anabolic steroids may also have low sex hormone binding globulin. Higher TRT dose (over 200 mg/week of T injections) may also decrease sex hormone binding globulin.
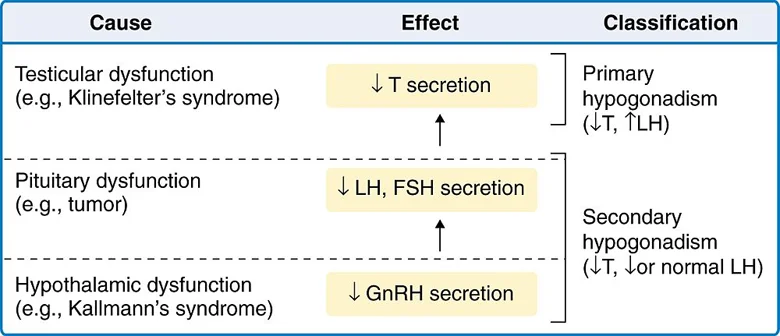
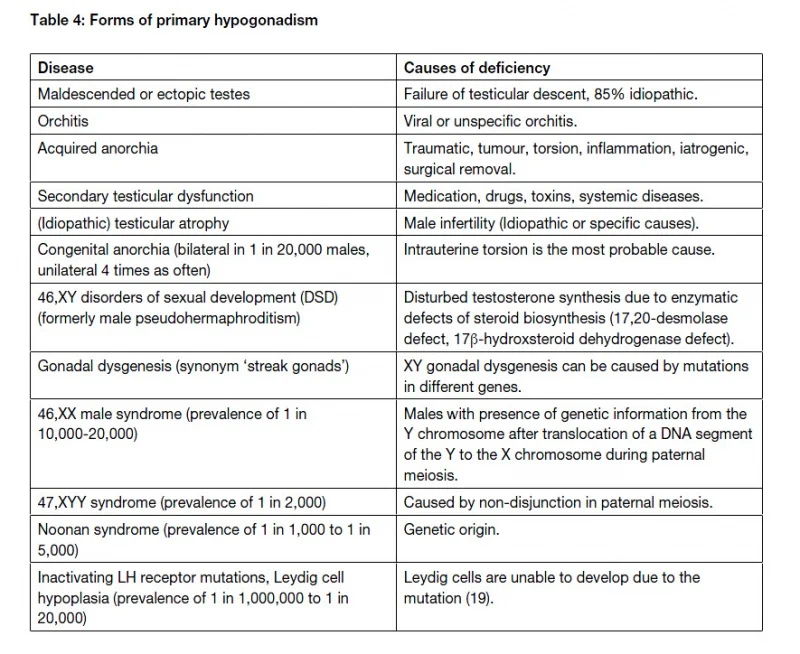
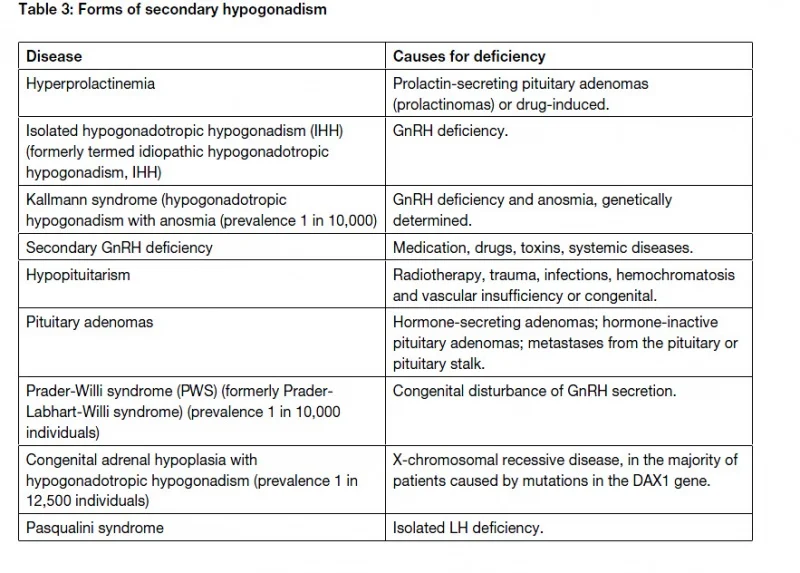
There are several types of hypogonadism depending on the level of LH, FSH and testosterone:
Conditions associated with alterations in sex hormone binding globulin (SHBG) concentrations and lower/higher free testosterone
Conditions associated with decreased SHBG concentrations
• Moderate obesity*
• Nephrotic syndrome*
• Hypothyroidism
• Use of glucocorticoids, progestins, and androgenic steroids*
• Acromegaly
• Diabetes mellitus*
Conditions associated with increased SHBG concentrations
• Aging*
• Hepatic cirrhosis and hepatitis*
• Hyperthyroidism
• Use of anticonvulsants*
• Use of estrogens
• HIV disease
* Particularly common conditions associated with alterations in SHBG concentrations
LH and FSH should be measured at baseline to document if hypogonadism is primary (Testicular-high LH and FSH and low T) or secondary (Pituitary- Low LH and/or FSH). LH and FSH are suppressed by TRT, so no need to measure at follow up.
If TT< 200 ng/dL, measure prolactin (out-of-pocket expense) to rule out prolactemia induced by pituitary adenoma. If prolactin is over 100 ng/mL, a referral to an endocrinologist is needed. Pituitary MRI and cabergoline treatment may be needed.
Note: Substantial elevation in prolactin (>150 ng/mL) usually indicates a pituitary tumor. Very high levels of prolactin are associated with larger tumors.
Modest levels of prolactin elevation (25–100 ng/mL) may be associated with the use of several medications. All other causes of hyperprolactinemia should be excluded before a tumor is considered. Primary hypothyroidism and chronic renal disease is associated with elevations in prolactin, probably because of altered metabolism or clearance of prolactin. The following medications can cause elevated prolactin and very low TT blood levels:
Prolactin: Should Men with Erectile Dysfunction Be Tested ?
Hypothyrodism (TSH>3.5 U/mL or below normal free T3) can lead to hypogonadism. If patient is experiencing cold intolerance in extremities, fatigue and weight gain TSH should be measured . Free T3 and T4, thyroid antibodies, and reverse T3 tests may be needed to determine the root cause of high TSH.
A digital-rectal exam (DRE) is recommended at baseline prior to starting testosterone replacement to document any BPH. BPH is not a contraindication but urinary track symptoms should be closely monitored to detect worsening due to TRT associated prostate volume increase. Prostate volume increases plateau after 4 months on TRT.
Physical exam should also include a list of medications taken by patient. Ketoconazole (current use), cimetidine (current use), opiates (current or prior use), anabolic steroids (current or prior use), glucocorticoids (current or prior use), finasteride (current or prior use), Accutane (current or prior use) and OTC supplements can decrease TT and FT levels. Hypertension medications like beta blockers and diuretics can decrease libido and worsen ED (ACE inhibitors may have a lower incidence for these issues). Antidepressants (exception: bupropion- Wellbutrin), anxiolytics, and statins have also been associated with lower libido, ED and/or orgasmic issues.
Traumatic head injury has been associated with low TT blood levels in young men, so please ensure that this is noted in chart if present.
CONTRAINDICATIONS TO TESTOSTERONE REPLACEMENT THERAPY
Patients with the following issues should not be treated with TRT unless issue is corrected:
1. Severe sleep apnea not treated with CPAP
2. Hematocrit > 50 (without TRT)
a. For patients with hematocrit > 50, inquire about recent testosterone or anabolic steroid use, sleep apnea, heavy smoking, or family history of congenital polycythemia or lung disease.
3. PSA> 4
NOTE:
a. Men with prior history of prostate cancer that has been successfully treated and whose PSA has remained stable over a year are not excluded from TRT.Testosterone Replacement in Men Treated for Prostate Cancer
b. If PSA increases by > 1 ng/mL or approaches 4 ng/mL by follow up visit, ensure that potential prostatitis is addressed. Increased sexual activity may also expose some men to higher risks of prostate infections. Inquire about potential symptoms of UTI.
c. If PSA does not decrease after 4 weeks of antibiotic treatment, a referral to urology is required. TRT cessation may be discussed with patient at that moment.
4. The FDA has sent a warning to inform that men with prior history of clotting disorders (DVT, etc) may have relapse on TRT . No studies have been performed to determine if blood thinners can enable a patient to start TRT safely. Two percent of men may have genetic mutations that predispose them to blood clots.Can Testosterone Induce Blood Clots and Thrombosis? Interview with Dr Charles Glueck
5. TRT is not contraindicated for obese patients and those with history of MI/CDV.
TRT DOSING:
Testosterone Cypionate Injections:
100 mg per week or 50 mg twice per week. Check TT and FT at follow up and titrate dose to achieve TT >600 ng/dL Max dose: 250 mg/week (or 125 mg twice per week). Injections are performed using a 26 or 27 gauge ½ inch insulin syringe subcutaneously on the abdominal area or intramuscularly on glutes, shoulders or hamstrings.
Compounded Testosterone Cream (2 %):
1 ml on shoulders or inner thighs after daily showering. Advise patient of risk of transferring testosterone to females or children during the first 12 hours of application.
TRT ADJUNCTIVE MEDICATIONS:
hCG (Human Chorionic Gonadotropin)- Compounded 11,000 IU vial
Approved for fertility and hypogonadism. Shown to prevent/reverse testicular atrophy and loss of fertility caused by TRT. Starting dose 350 IU twice per week subcutaneously. If no improvement in testicular size is reported by patient, dose can be increased to 500 IU twice per week. Patient can chose to combine hCG plus T cypionate in same syringe twice per week ( 50-75 mg of T cypionate plus 350-500 IU hCG twice per week). hCG is water soluble and T cypionate is oil based, so they do not mix. You can chose to offer hCG at baseline or at follow up depending on patient’s need to remain fertile and/or concerns of testicular atrophy.
ExcelMale.com suggests simplifying injection frequency with this protocol:
Video: How to Use HCG with Testosterone To Preserve Fertility, Libido and Testicle Size
Anastrozole – Compounded 0.25 mg, 0.5 mg or 1 mg capsules.
This drug inhibits aromatase activity. Prescribed only if patient has a sensitive estradiol value over 50 pg/ml at follow up. Starting dose is 0.5 mg per week. If sensitive estradiol is >50 pg/ml at second follow up, increase dose to a maximum of 1 mg/week. Caution: Low estradiol of 20 ng/mL or below has been associated with low libido, bone loss and higher fat gains. Very high estradiol may cause gynecomastia specially in the presence of low testosterone (low T/E ratio).
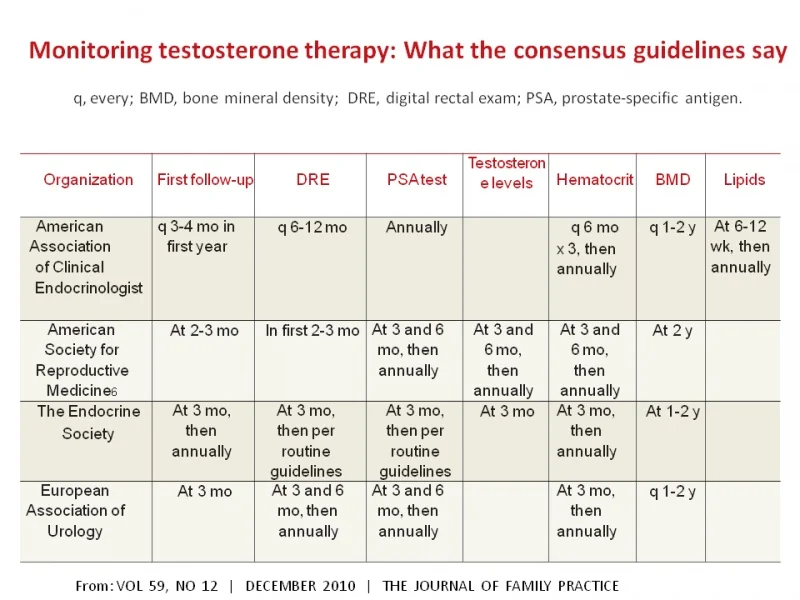
BLOOD TEST MONITORING SCHEDULE
The monitoring guidelines of ExcelMale.com are more strict than all current TRT medical guidelines. You can see a summary of blood testing and examinations required by the main four medical groups in this table.
Bone mineral density (by DEXA) is not usually included in monitoring schedule since it may be only an important variable only for men with ages 65 and over. TRT increases BMD and lowers the risk of fractures.
The following are the required blood tests and how to use them for clinical decision making. You can get them cheaply in most U.S. cities here

• Initial Blood Test – New Patient
– Testosterone, Free & Total
– PSA
– LH & FSH
– Lipids
– CBC
– CMP
-Free T3
-Sensitive Estradiol
If T <200 ng/dL and no current/past use of anabolics or opiates, test for prolactin.
If free T3 is low, perform a complete thyroid panel including antibodies and reverse T3.
• Initial Blood Test – Transferring Patient from one clinic to another (currently on testosterone or has been in last 3 months)
Fasted, morning and well hydrated conditions:
– Testosterone, Free & Total
– PSA
– LH & FSH
– Lipids
– CBC
– CMP
– Estradiol, sensitive
– Free T3
• 6wk Follow up – 6wks after initial Rx
Fasted, morning sample and well hydrated conditions:
– CBC
– CMP
– Testosterone, Free & Total
– Estradiol, sensitive
– Free T3
• 6 Month Follow up – 6 months after initial RX
– Testosterone, Free & Total
– PSA (optional based on week 6 results)
– Lipids
– CBC
– CMP
– Estradiol, sensitive
– Free T3 (if abnormal FT3 was found at baseline and thyroid treatment was provided)
• Annual Blood Test – Same as 6 months (plus PSA)
MANAGEMENT OF KEY TRT VARIABLES:
At follow up:
Adjust TRT , hCG and/or anastrozole dose if needed based on blood test values and symptoms. If total testosterone (TT) has decreased from week 6, investigate patient treatment adherence.
If patient has a TT >600 ng/dL and still fatigued, check TSH and free T3 (out-of-pocket) and inquire about sleep apnea symptoms. If TT <600 ng/dL, increase T dose by 50%. Some men are fast metabolizers of testosterone. Adherence to TRT should be investigated if TT < 500 ng/dL.
You may increase the initial hCG dose from 350 IU to 500 IU if patient reports low libido even with TT> 600 ng/dL. Increased hCG dose may also increase DHT, an important metabolite linked to libido. Most patients do not complain about testicular atrophy with these hCG doses.
Very low HDL (< 35 mg/dL) may indicate high T dose or anabolic steroid use. Triglycerides usually decrease with TRT. LDL may decrease to a smaller degree.
If hematocrit approaches 52, please advise patient to donate blood every two to three months with careful monitoring of ferritin levels to avoid depletion that can cause fatigue. If patient is excluded from donation due to not meeting health requirements, it is advised to write an order for patient to take to a blood center. Out-of-pocket expense may be required.
If estradiol > 50 pg/mL, start patient on .5 mg per week of anastrozole. At week 6 follow up titrate dose of anastrozole so that estradiol is not under 20 pg/mL. Most men do not need anastrozole unless they have a high BMI (fat content) or liver disease.
If eGFR <65 or liver enzymes > 20 percent of max , ask patient if they have started any supplements like creatine or others that can affect kidney or liver function heavy exercisers and high protein consumers may also have higher creatinine and AST and ALT. This higher levels are non-clinical significant and should be documented in chart.
If you can’t read the above table, click here
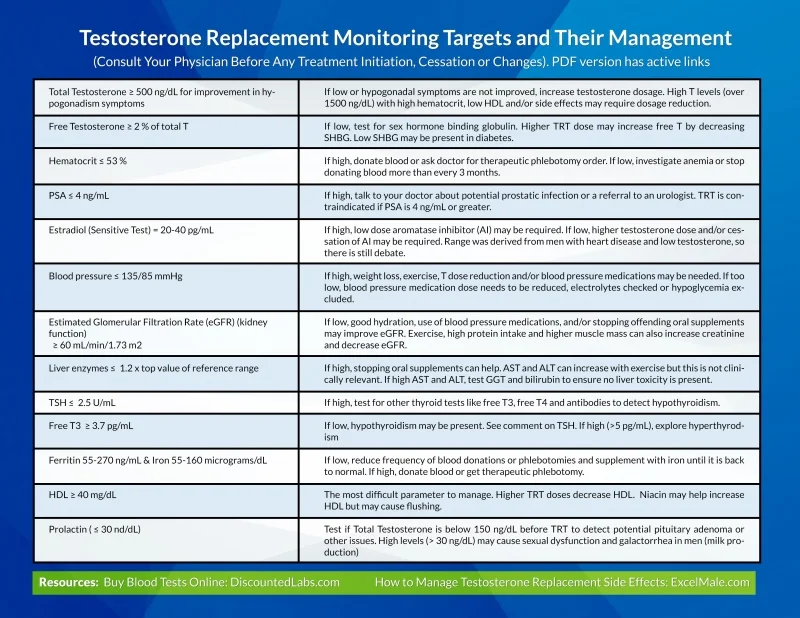
SIDE EFFECT MANAGEMENT:
Please refer to this table for details on side effect management:
Testosterone Side Effect Management Table
SPECIAL POPULATIONS
1- Patients with BMI> 28 with high fat percent. These patients may aromatize testosterone more than lean patients, so their estradiol may be higher than normal. They may need anastrozole at week 6. As weight decreases with TRT (assuming they have also engaged in life style improvements), their testosterone aromatization may decrease and so will their need for anastrozole. Obese patients may also present with sleep apnea and metabolic syndrome (high triglycerides, low HDL, high fasted glucose). Their lipids and glucose may improve on TRT but sleep apnea may worsen, so they may actually feel worse on TRT unless they use a CPAP machine.
2- Patients with previous history of clotting disorders. A small study showed that men with previous deep vain thrombosis and clotting issues (2 percent of men in a large cohort) may be predisposed to relapse of clotting on TRT. They may have genetic mutations that predispose them to clotting. It is important to identify these patients at baseline. They should not be provided TRT due to risks. Patients with this risk should refer to Dr Charles Glueck, the lead author of that study who is currently looking for more of these patients to test them for genetic mutations. Can Testosterone Induce Blood Clots and Thrombosis? Interview with Dr Charles Glueck
3- TRT is not contraindicated for patients with diabetes or history of MI or CVD.
The post Diagnosis and Management of Hypogonadism (Low Testosterone) appeared first on Testosterone Wisdom.
Continue reading...
Diagnosis and Management of Hypogonadism
DIAGNOSIS OF HYPOGONADISM:
Symptoms and signs suggestive of testosterone deficiency in men:
A. More specific symptoms and signs
• Incomplete or delayed sexual development, eunuchoidism
• Reduced sexual desire (libido) and activity
• Decreased spontaneous erections during sleep
• Breast discomfort, gynecomastia
• Loss of body (axillary and pubic) hair, reduced shaving
• Very small (especially <5 ml) or shrinking testes
• Inability to father children, low or zero sperm count
• Height loss, low trauma fracture, low bone mineral density
• Hot flashes, sweats
B. Other less specific symptoms and signs
• Decreased energy, motivation, initiative, and self-confidence
• Feeling sad or blue, depressed mood, dysthymia
• Poor concentration and memory
· Decreased penile sensitivity
• Sleep disturbance, increased sleepiness
• Mild anemia (normochromic, normocytic, in the female range)
• Reduced muscle bulk and strength
• Increased body fat, body mass index
• Diminished physical or work performance
ADAM questionnaire about symptoms of low testosterone
(Androgen Deficiency in the Aging Male)
This basic questionnaire can be very useful for men to describe the kind and severity of their low testosterone symptoms.
1. Do you have a decrease in libido (sex drive)? Yes No
2. Do you have a lack of energy? Yes No
3. Do you have a decrease in strength and/or endurance? Yes No
4. Have you lost height? Yes No
5. Have you noticed a decreased “enjoyment of life” Yes No
6. Are you sad and/or grumpy? Yes No
7. Are your erections less strong? Yes No
8. Have you noticed a recent deterioration in your ability to play sports? Yes No
9. Are you falling asleep after dinner? Yes No
10. Has there been a recent deterioration in your work performance? Yes No
If patient answers Yes to number 1 or 7 or if he answers Yes to more than 3 questions, he may have hypogonadism.
Blood Tests and Physical Exam:
Total testosterone (TT) blood level of 400 ng/dL or below along with hypogonadism symptoms not caused by temporary factors (lack of sleep, recent excess weight gain, thyroid dysfunction, temporary illness, and anabolic steroid use). For men with TT > 400 ng/dL, lifestyle modification counseling to lower BMI (If BMI >26), improve sleep hygiene, and exercise is recommended. These are other interventions that may increase testosterone in men: How to Increase Testosterone Naturally
Free Testosterone (FT) blood levels should be at least 2 percent of TT. Not much can be done to manipulate sex hormone binding globulin (SHBG) to increase FT levels since it may be determined by genetics, comorbidities, insulin or inflammation. People with diabetes and hyperglycemia may have lower levels of sex hormone binding globulin even in the presence of low TT. Men on anabolic steroids may also have low sex hormone binding globulin. Higher TRT dose (over 200 mg/week of T injections) may also decrease sex hormone binding globulin.
There are several types of hypogonadism depending on the level of LH, FSH and testosterone:
Conditions associated with alterations in sex hormone binding globulin (SHBG) concentrations and lower/higher free testosterone
Conditions associated with decreased SHBG concentrations
• Moderate obesity*
• Nephrotic syndrome*
• Hypothyroidism
• Use of glucocorticoids, progestins, and androgenic steroids*
• Acromegaly
• Diabetes mellitus*
Conditions associated with increased SHBG concentrations
• Aging*
• Hepatic cirrhosis and hepatitis*
• Hyperthyroidism
• Use of anticonvulsants*
• Use of estrogens
• HIV disease
* Particularly common conditions associated with alterations in SHBG concentrations
LH and FSH should be measured at baseline to document if hypogonadism is primary (Testicular-high LH and FSH and low T) or secondary (Pituitary- Low LH and/or FSH). LH and FSH are suppressed by TRT, so no need to measure at follow up.
If TT< 200 ng/dL, measure prolactin (out-of-pocket expense) to rule out prolactemia induced by pituitary adenoma. If prolactin is over 100 ng/mL, a referral to an endocrinologist is needed. Pituitary MRI and cabergoline treatment may be needed.
Note: Substantial elevation in prolactin (>150 ng/mL) usually indicates a pituitary tumor. Very high levels of prolactin are associated with larger tumors.
Modest levels of prolactin elevation (25–100 ng/mL) may be associated with the use of several medications. All other causes of hyperprolactinemia should be excluded before a tumor is considered. Primary hypothyroidism and chronic renal disease is associated with elevations in prolactin, probably because of altered metabolism or clearance of prolactin. The following medications can cause elevated prolactin and very low TT blood levels:
Prolactin: Should Men with Erectile Dysfunction Be Tested ?
Hypothyrodism (TSH>3.5 U/mL or below normal free T3) can lead to hypogonadism. If patient is experiencing cold intolerance in extremities, fatigue and weight gain TSH should be measured . Free T3 and T4, thyroid antibodies, and reverse T3 tests may be needed to determine the root cause of high TSH.
A digital-rectal exam (DRE) is recommended at baseline prior to starting testosterone replacement to document any BPH. BPH is not a contraindication but urinary track symptoms should be closely monitored to detect worsening due to TRT associated prostate volume increase. Prostate volume increases plateau after 4 months on TRT.
Physical exam should also include a list of medications taken by patient. Ketoconazole (current use), cimetidine (current use), opiates (current or prior use), anabolic steroids (current or prior use), glucocorticoids (current or prior use), finasteride (current or prior use), Accutane (current or prior use) and OTC supplements can decrease TT and FT levels. Hypertension medications like beta blockers and diuretics can decrease libido and worsen ED (ACE inhibitors may have a lower incidence for these issues). Antidepressants (exception: bupropion- Wellbutrin), anxiolytics, and statins have also been associated with lower libido, ED and/or orgasmic issues.
Traumatic head injury has been associated with low TT blood levels in young men, so please ensure that this is noted in chart if present.
CONTRAINDICATIONS TO TESTOSTERONE REPLACEMENT THERAPY
Patients with the following issues should not be treated with TRT unless issue is corrected:
1. Severe sleep apnea not treated with CPAP
2. Hematocrit > 50 (without TRT)
a. For patients with hematocrit > 50, inquire about recent testosterone or anabolic steroid use, sleep apnea, heavy smoking, or family history of congenital polycythemia or lung disease.
3. PSA> 4
NOTE:
a. Men with prior history of prostate cancer that has been successfully treated and whose PSA has remained stable over a year are not excluded from TRT.Testosterone Replacement in Men Treated for Prostate Cancer
b. If PSA increases by > 1 ng/mL or approaches 4 ng/mL by follow up visit, ensure that potential prostatitis is addressed. Increased sexual activity may also expose some men to higher risks of prostate infections. Inquire about potential symptoms of UTI.
c. If PSA does not decrease after 4 weeks of antibiotic treatment, a referral to urology is required. TRT cessation may be discussed with patient at that moment.
4. The FDA has sent a warning to inform that men with prior history of clotting disorders (DVT, etc) may have relapse on TRT . No studies have been performed to determine if blood thinners can enable a patient to start TRT safely. Two percent of men may have genetic mutations that predispose them to blood clots.Can Testosterone Induce Blood Clots and Thrombosis? Interview with Dr Charles Glueck
5. TRT is not contraindicated for obese patients and those with history of MI/CDV.
TRT DOSING:
Testosterone Cypionate Injections:
100 mg per week or 50 mg twice per week. Check TT and FT at follow up and titrate dose to achieve TT >600 ng/dL Max dose: 250 mg/week (or 125 mg twice per week). Injections are performed using a 26 or 27 gauge ½ inch insulin syringe subcutaneously on the abdominal area or intramuscularly on glutes, shoulders or hamstrings.
Compounded Testosterone Cream (2 %):
1 ml on shoulders or inner thighs after daily showering. Advise patient of risk of transferring testosterone to females or children during the first 12 hours of application.
TRT ADJUNCTIVE MEDICATIONS:
hCG (Human Chorionic Gonadotropin)- Compounded 11,000 IU vial
Approved for fertility and hypogonadism. Shown to prevent/reverse testicular atrophy and loss of fertility caused by TRT. Starting dose 350 IU twice per week subcutaneously. If no improvement in testicular size is reported by patient, dose can be increased to 500 IU twice per week. Patient can chose to combine hCG plus T cypionate in same syringe twice per week ( 50-75 mg of T cypionate plus 350-500 IU hCG twice per week). hCG is water soluble and T cypionate is oil based, so they do not mix. You can chose to offer hCG at baseline or at follow up depending on patient’s need to remain fertile and/or concerns of testicular atrophy.
ExcelMale.com suggests simplifying injection frequency with this protocol:
Video: How to Use HCG with Testosterone To Preserve Fertility, Libido and Testicle Size
Anastrozole – Compounded 0.25 mg, 0.5 mg or 1 mg capsules.
This drug inhibits aromatase activity. Prescribed only if patient has a sensitive estradiol value over 50 pg/ml at follow up. Starting dose is 0.5 mg per week. If sensitive estradiol is >50 pg/ml at second follow up, increase dose to a maximum of 1 mg/week. Caution: Low estradiol of 20 ng/mL or below has been associated with low libido, bone loss and higher fat gains. Very high estradiol may cause gynecomastia specially in the presence of low testosterone (low T/E ratio).
BLOOD TEST MONITORING SCHEDULE
The monitoring guidelines of ExcelMale.com are more strict than all current TRT medical guidelines. You can see a summary of blood testing and examinations required by the main four medical groups in this table.
Bone mineral density (by DEXA) is not usually included in monitoring schedule since it may be only an important variable only for men with ages 65 and over. TRT increases BMD and lowers the risk of fractures.
The following are the required blood tests and how to use them for clinical decision making. You can get them cheaply in most U.S. cities here
• Initial Blood Test – New Patient
– Testosterone, Free & Total
– PSA
– LH & FSH
– Lipids
– CBC
– CMP
-Free T3
-Sensitive Estradiol
If T <200 ng/dL and no current/past use of anabolics or opiates, test for prolactin.
If free T3 is low, perform a complete thyroid panel including antibodies and reverse T3.
• Initial Blood Test – Transferring Patient from one clinic to another (currently on testosterone or has been in last 3 months)
Fasted, morning and well hydrated conditions:
– Testosterone, Free & Total
– PSA
– LH & FSH
– Lipids
– CBC
– CMP
– Estradiol, sensitive
– Free T3
• 6wk Follow up – 6wks after initial Rx
Fasted, morning sample and well hydrated conditions:
– CBC
– CMP
– Testosterone, Free & Total
– Estradiol, sensitive
– Free T3
• 6 Month Follow up – 6 months after initial RX
– Testosterone, Free & Total
– PSA (optional based on week 6 results)
– Lipids
– CBC
– CMP
– Estradiol, sensitive
– Free T3 (if abnormal FT3 was found at baseline and thyroid treatment was provided)
• Annual Blood Test – Same as 6 months (plus PSA)
MANAGEMENT OF KEY TRT VARIABLES:
At follow up:
Adjust TRT , hCG and/or anastrozole dose if needed based on blood test values and symptoms. If total testosterone (TT) has decreased from week 6, investigate patient treatment adherence.
If patient has a TT >600 ng/dL and still fatigued, check TSH and free T3 (out-of-pocket) and inquire about sleep apnea symptoms. If TT <600 ng/dL, increase T dose by 50%. Some men are fast metabolizers of testosterone. Adherence to TRT should be investigated if TT < 500 ng/dL.
You may increase the initial hCG dose from 350 IU to 500 IU if patient reports low libido even with TT> 600 ng/dL. Increased hCG dose may also increase DHT, an important metabolite linked to libido. Most patients do not complain about testicular atrophy with these hCG doses.
Very low HDL (< 35 mg/dL) may indicate high T dose or anabolic steroid use. Triglycerides usually decrease with TRT. LDL may decrease to a smaller degree.
If hematocrit approaches 52, please advise patient to donate blood every two to three months with careful monitoring of ferritin levels to avoid depletion that can cause fatigue. If patient is excluded from donation due to not meeting health requirements, it is advised to write an order for patient to take to a blood center. Out-of-pocket expense may be required.
If estradiol > 50 pg/mL, start patient on .5 mg per week of anastrozole. At week 6 follow up titrate dose of anastrozole so that estradiol is not under 20 pg/mL. Most men do not need anastrozole unless they have a high BMI (fat content) or liver disease.
If eGFR <65 or liver enzymes > 20 percent of max , ask patient if they have started any supplements like creatine or others that can affect kidney or liver function heavy exercisers and high protein consumers may also have higher creatinine and AST and ALT. This higher levels are non-clinical significant and should be documented in chart.
If you can’t read the above table, click here
SIDE EFFECT MANAGEMENT:
Please refer to this table for details on side effect management:
Testosterone Side Effect Management Table
SPECIAL POPULATIONS
1- Patients with BMI> 28 with high fat percent. These patients may aromatize testosterone more than lean patients, so their estradiol may be higher than normal. They may need anastrozole at week 6. As weight decreases with TRT (assuming they have also engaged in life style improvements), their testosterone aromatization may decrease and so will their need for anastrozole. Obese patients may also present with sleep apnea and metabolic syndrome (high triglycerides, low HDL, high fasted glucose). Their lipids and glucose may improve on TRT but sleep apnea may worsen, so they may actually feel worse on TRT unless they use a CPAP machine.
2- Patients with previous history of clotting disorders. A small study showed that men with previous deep vain thrombosis and clotting issues (2 percent of men in a large cohort) may be predisposed to relapse of clotting on TRT. They may have genetic mutations that predispose them to clotting. It is important to identify these patients at baseline. They should not be provided TRT due to risks. Patients with this risk should refer to Dr Charles Glueck, the lead author of that study who is currently looking for more of these patients to test them for genetic mutations. Can Testosterone Induce Blood Clots and Thrombosis? Interview with Dr Charles Glueck
3- TRT is not contraindicated for patients with diabetes or history of MI or CVD.
The post Diagnosis and Management of Hypogonadism (Low Testosterone) appeared first on Testosterone Wisdom.
Continue reading...











