My Prolactin is a bit high at 448 and the UK range is 86-324 mU/L. One doc said to me its not a problem another said I should take Cabergoline to lower it at 0.25mg twice a week. I wondered what is the benefit to lowering it to what level for us on TRT. I was told its normal to have high Prolactin on TRT?. Do we feel any better if it is lower, I did read that high Prolactin can increase fat round the middle, I must say I find it hard to shift the love handles , whether we can blame that on Prolactin I dont know and how high does it have to be to cause fat. I also wonder if it someway interferes with the efficiency of T etc. In other words whats wrong with having slightly elevated Prolactin.?

- Forums
- Thyroid, Pregnenolone, Progesterone, DHEA, etc
- Thyroid, DHEA, Pregnenolone, Progesterone, etc
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
When is Prolactin too high and what are benefits of lowering it
- Category Hormones
- Category Men's Health

Primobolan decreases E2. Forget the exact mechanism by which it does this, but most DHT derivatives will lower E2 in ur serum and on a blood test, or inhibit E2‘s effects, but won’t visibly show a lowering of E2 on a blood test. Masteron is an example of inhibiting E2’s effects, but not lowering E2 in the serum/ on a blood test. It was initially created to treat breast cancer. Hence the prefix “mast”. They studied it in this regard due to its inhibition of E2. Primobolan actually lowers E2 in the serum, and since E2 is the main stimulator of prolactin release in the male body, prolactin will subsequently tend to go down as E2 goes down.
See my comments in the context of your message above:
Gman86: Primobolan decreases E2. Forget the exact mechanism by which it does this, but most DHT derivatives will lower E2 in ur serum and on a blood test, or inhibit E2‘s effects, but won’t visibly show a lowering of E2 on a blood test.
ss: If most DHT derivatives will lower E2 but not show it on a blood test then I cannot conclude the first part of your contradictory statement above. It just makes no sense.
And, the peer-reviewed literature on primobolan is so scant and so old that no article I can find discusses primobolan vs. E2. Moreover, despite this being an interesting hormone (Methenolone Acetate), it appears that a reliable source of it in the US and most of Europe is not the case.
Gman86: Masteron is an example of inhibiting E2’s effects, but not lowering E2 in the serum/ on a blood test. It was initially created to treat breast cancer. Hence the prefix “mast”.
ss: this is another very old drug that has scant literature on it. The chemical name is drostanolone proprionate. The articles I found dated 1970 to 1987 with most from the 70s. I was treating breast cancer in the '70s and never came across this drug in the US. One paper from 2020 is Borodi, G.; Turza, A.; Bende, A. Exploring the Polymorphism of Drostanolone Propionate. Molecules 2020, 25, doi:10.3390/molecules25061436. Here is the abstract:
2alpha-Methyl-4,5alpha-dihydrotestosterone 17beta-propionate, known as drostanolone propionate or masteron, is a synthetic anabolic-androgenic steroid derived from dihydrotestosterone. The crystal structures of two polymorphs of drostanolone propionate have been determined by single crystal X-ray diffraction and both crystallizes in the monoclinic crystal system. One is belonging to the P2(1) space group, Z = 2, and has one molecule in the asymmetric unit while the second belongs to the I2 space group, Z = 4, and contains two molecules in the asymmetric unit. Another polymorph has been investigated by an X-ray powder diffraction method and solved by Parallel tempering/Monte Carlo technique and refined with the Rietveld method. This polymorph crystallizes in the orthorhombic P2(1)2(1)2(1) space group, Z = 4 having one molecule in the asymmetric unit. The structural configuration analysis shows that the A, B, and C steroid rings exist as chair geometry, while ring D adopts a C13 distorted envelope configuration in all structures. For all polymorphs, the lattice energy has been computed by CLP (Coulomb-London-Pauli), and tight-binding density functional theory methods. Local electron correlation methods were used to estimate the role of electron correlation in the magnitude of the dimer energies. The nature of the intermolecular interactions has been analyzed by the SAPT0 energy decomposition methods as well as by Hirshfeld surfaces.
As you can see, this publication has little human clinical relevance; at least not to me as a medical oncologist. I do not know how you have information on Masteron (aka Masteril).
One of the papers I obtained from 1970 (Treatment of Advanced Breast Carcinoma Treatment of Advanced Breast Carcinoma with with Drostanolone Propionate) had only this to say regarding mechanism of action:
Deshpanda (1967) demonstrated that drostanolone propionate reduced the uptake of oestradiol-17B by tumour cells, reduced the uptake of oestradiol-17B by tumour cells, whereas Altman and Chayen (1967) suggested that whereas Altman and Chayen (1967) suggested that the drug acted by diverting the reduced co-enzyme the drug acted by diverting the reduced co-enzyme NADPH into the metabolically wasteful diaphorase NADPH thus limiting the amount of biosynthesis in the carcinoma.}. None of the other paper's titles appear to address aromatization.
Gman86: They studied it in this regard due to its inhibition of E2.
ss: assuming you are referring to drostanolone. I purchased one paper that might shed clues on the mechanism of action of drostanolone (Masteron, Masteril, Masterid).
Trams, G. Effect of drostanolone propionate on the binding of oestradiol and dihydrotestosterone by normal and malignant target tissues. Eur J Cancer (1965) 1977, 13, 149-153, doi:10.1016/0014-2964(77)90193-1
Drostanolone was.found to compete with androgen binding sites but not with oestrogen receptors. Therefore it is unlikely that the growth inhibitory effect of drostanolone propionate in human breast cancer is mediated through interaction with oestradiol binding proteins as suggested earlier by other authors.
Sorry, but unless you come up with some validation of your statements, it appears that you are presenting your own opinions, and not facts as we think we known them.
Gman86: Primobolan actually lowers E2 in the serum, and since E2 is the main stimulator of prolactin release in the male body, prolactin will subsequently tend to go down as E2 goes down.
ss: Primobolan (aka methenolone acetate) is an anaobolic steroid. Like DHT and T it stimulates the AR (androgen receptor). By raising T and DHT, it might reflexly ↓ E2. But I cannot find any articles to that effect. Please share such articles with us. I have not found in my use of androgen deprivation therapy (ADT) in thousands of men, a decrease in prolactin and have had to use a prolactin inhibitor like cabergoline (Dostinex®) to achieve lowering. There is a reflex inter-relationship between prolactin and dopamine but I have not seen this to be the case between raising T ⇢ lowering E2 ⇢ lowering prolactin . You sound convincing so maybe you have the articles to support this. I share two articles I referred to above.
Stephen B. Strum, MD, FACP
Attachments

DHT as aromatase inhibitor:

 pubmed.ncbi.nlm.nih.gov
DHT acting on ER through competitive inhibition:
pubmed.ncbi.nlm.nih.gov
DHT acting on ER through competitive inhibition:
pubmed.ncbi.nlm.nih.gov
FSH-induced aromatase activity in porcine granulosa cells: non-competitive inhibition by non-aromatizable androgens - PubMed
The aim of this study was to examine the inhibitory effect of the non-aromatizable androgens on FSH-stimulated aromatase activity in porcine granulosa cells. The cells were isolated from medium-sized follicles (4-6 mm) of prepubertal pigs, and cultured under chemically defined conditions in the...
pubmed.ncbi.nlm.nih.gov
Antiestrogenic action of dihydrotestosterone in mouse breast. Competition with estradiol for binding to the estrogen receptor - PubMed
Feminization in men occurs when the effective ratio of androgen to estrogen is lowered. Since sufficient estrogen is produced in normal men to induce breast enlargement in the absence of adequate amounts of circulating androgens, it has been generally assumed that androgens exert an...
pubmed.ncbi.nlm.nih.gov
Im not a big study guy. Im more of a real world results/ anecdotes guy. I care more about what is actually happening to guys when using these compounds, vs what flawed/ corrupt studies tell us what should happen. But it’s important to have people like u that put more weight into study results. So I definitely can appreciate the way u approach these thingsSee my comments in the context of your message above:
Gman86: Primobolan decreases E2. Forget the exact mechanism by which it does this, but most DHT derivatives will lower E2 in ur serum and on a blood test, or inhibit E2‘s effects, but won’t visibly show a lowering of E2 on a blood test.
ss: If most DHT derivatives will lower E2 but not show it on a blood test then I cannot conclude the first part of your contradictory statement above. It just makes no sense.
And, the peer-reviewed literature on primobolan is so scant and so old that no article I can find discusses primobolan vs. E2. Moreover, despite this being an interesting hormone (Methenolone Acetate), it appears that a reliable source of it in the US and most of Europe is not the case.
Gman86: Masteron is an example of inhibiting E2’s effects, but not lowering E2 in the serum/ on a blood test. It was initially created to treat breast cancer. Hence the prefix “mast”.
ss: this is another very old drug that has scant literature on it. The chemical name is drostanolone proprionate. The articles I found dated 1970 to 1987 with most from the 70s. I was treating breast cancer in the '70s and never came across this drug in the US. One paper from 2020 is Borodi, G.; Turza, A.; Bende, A. Exploring the Polymorphism of Drostanolone Propionate. Molecules 2020, 25, doi:10.3390/molecules25061436. Here is the abstract:
2alpha-Methyl-4,5alpha-dihydrotestosterone 17beta-propionate, known as drostanolone propionate or masteron, is a synthetic anabolic-androgenic steroid derived from dihydrotestosterone. The crystal structures of two polymorphs of drostanolone propionate have been determined by single crystal X-ray diffraction and both crystallizes in the monoclinic crystal system. One is belonging to the P2(1) space group, Z = 2, and has one molecule in the asymmetric unit while the second belongs to the I2 space group, Z = 4, and contains two molecules in the asymmetric unit. Another polymorph has been investigated by an X-ray powder diffraction method and solved by Parallel tempering/Monte Carlo technique and refined with the Rietveld method. This polymorph crystallizes in the orthorhombic P2(1)2(1)2(1) space group, Z = 4 having one molecule in the asymmetric unit. The structural configuration analysis shows that the A, B, and C steroid rings exist as chair geometry, while ring D adopts a C13 distorted envelope configuration in all structures. For all polymorphs, the lattice energy has been computed by CLP (Coulomb-London-Pauli), and tight-binding density functional theory methods. Local electron correlation methods were used to estimate the role of electron correlation in the magnitude of the dimer energies. The nature of the intermolecular interactions has been analyzed by the SAPT0 energy decomposition methods as well as by Hirshfeld surfaces.
As you can see, this publication has little human clinical relevance; at least not to me as a medical oncologist. I do not know how you have information on Masteron (aka Masteril).
One of the papers I obtained from 1970 (Treatment of Advanced Breast Carcinoma Treatment of Advanced Breast Carcinoma with with Drostanolone Propionate) had only this to say regarding mechanism of action:
Deshpanda (1967) demonstrated that drostanolone propionate reduced the uptake of oestradiol-17B by tumour cells, reduced the uptake of oestradiol-17B by tumour cells, whereas Altman and Chayen (1967) suggested that whereas Altman and Chayen (1967) suggested that the drug acted by diverting the reduced co-enzyme the drug acted by diverting the reduced co-enzyme NADPH into the metabolically wasteful diaphorase NADPH thus limiting the amount of biosynthesis in the carcinoma.}. None of the other paper's titles appear to address aromatization.
Gman86: They studied it in this regard due to its inhibition of E2.
ss: assuming you are referring to drostanolone. I purchased one paper that might shed clues on the mechanism of action of drostanolone (Masteron, Masteril, Masterid).
Trams, G. Effect of drostanolone propionate on the binding of oestradiol and dihydrotestosterone by normal and malignant target tissues. Eur J Cancer (1965) 1977, 13, 149-153, doi:10.1016/0014-2964(77)90193-1
Drostanolone was.found to compete with androgen binding sites but not with oestrogen receptors. Therefore it is unlikely that the growth inhibitory effect of drostanolone propionate in human breast cancer is mediated through interaction with oestradiol binding proteins as suggested earlier by other authors.
Sorry, but unless you come up with some validation of your statements, it appears that you are presenting your own opinions, and not facts as we think we known them.
Gman86: Primobolan actually lowers E2 in the serum, and since E2 is the main stimulator of prolactin release in the male body, prolactin will subsequently tend to go down as E2 goes down.
ss: Primobolan (aka methenolone acetate) is an anaobolic steroid. Like DHT and T it stimulates the AR (androgen receptor). By raising T and DHT, it might reflexly ↓ E2. But I cannot find any articles to that effect. Please share such articles with us. I have not found in my use of androgen deprivation therapy (ADT) in thousands of men, a decrease in prolactin and have had to use a prolactin inhibitor like cabergoline (Dostinex®) to achieve lowering. There is a reflex inter-relationship between prolactin and dopamine but I have not seen this to be the case between raising T ⇢ lowering E2 ⇢ lowering prolactin . You sound convincing so maybe you have the articles to support this. I share two articles I referred to above.
Stephen B. Strum, MD, FACP
I‘m not really sure what ur trying to say, in regards to masteron and breast cancer. All I know is Masteron was trialed on breast cancer patients. Like I said, that’s where the prefix “mast” comes from. If ur research reveals something different, we have to agree to disagree. But a quick google search will pull up multiple studies on the subject. So I’m not sure how it’s even arguable that at one point masteron was used in breast cancer patients. It’s not a current treatment for breast cancer, at least not that I’m aware of, so clearly it either wasn’t that great at treating breast cancer, or there wasn’t enough money in it to compete with modern methods to treat breast cancer that are much more profitable.
And idk what the studies on primo show. All I know is everyone that takes it will see a drop in E2. Obv that drop is going to be dependent on how many mgs of primo they’re using. For me personally, it’s a pretty potent ai. And that’s what I usually see in bloodwork from other men using it as well. Some men obv see less E2 inhibition than others. But everyone that I’ve seen use it has seen E2 decrease to some degree in their labs
and idk what studies show, but anecdotal reports and bloodwork that I’ve seen tends to show that prolactin follows E2. So when E2 goes up, prolactin in bloodwork tends to rise as well. And when E2 decreases in bloodwork, I tend to see prolactin drop as well.
If studies show u different things than what men are seeing anecdotally when using these compounds, we just have to agree to disagree, and that’s ok imo.
What’s scary are some clinical trials designed by doctors who have no idea how to achieve youthful hormone levels. The Travese study maintained 300-400 ng/dL total testosterone levels on androgel.Im more of a real world results/ anecdotes guy. I care more about what is actually happening to guys when using these compounds, vs what flawed/ corrupt studies tell us what should happen.
Not exactly youthful hormone levels.
Here's another thread that may interest you.DHT as aromatase inhibitor:
DHT acting on ER through competitive inhibition:FSH-induced aromatase activity in porcine granulosa cells: non-competitive inhibition by non-aromatizable androgens - PubMed
The aim of this study was to examine the inhibitory effect of the non-aromatizable androgens on FSH-stimulated aromatase activity in porcine granulosa cells. The cells were isolated from medium-sized follicles (4-6 mm) of prepubertal pigs, and cultured under chemically defined conditions in the...
Antiestrogenic action of dihydrotestosterone in mouse breast. Competition with estradiol for binding to the estrogen receptor - PubMed
Feminization in men occurs when the effective ratio of androgen to estrogen is lowered. Since sufficient estrogen is produced in normal men to induce breast enlargement in the absence of adequate amounts of circulating androgens, it has been generally assumed that androgens exert an...
A great example of what I’m referring to when I say that most studies are flawed, in some form or fashion. It’s not a conspiracy theory or anything. If u truly look at most studies, u can usually always find flaws in them somewhere. The issue then becomes how drastically are the results of the study tainted because of these flaws.What’s scary are some clinical trials designed by doctors who have no idea how to achieve youthful hormone levels. The Travese study maintained 300-400 ng/dL total testosterone levels on androgel.
Not exactly youthful hormone levels.
And then u still have the issue of corruption, which is unfortunately extremely common as well. But just like with government, I don’t blame individual politicians. I blame the corrupt political system that’s been in place way before any of the current politicians got into office. It’s the same with studies, imo. I blame the milieu that studies have to work within. There’s too much incentive to skew results, in order to improve one’s position within the ranks of their occupation, make a school or other facility look good, increase funding, provide results that allow something to be approved to be sold, etc. There’s just too much incentive for corruption. For the people running the studies, as well as the people overseeing studies.
But I digress lol. Studies obv have their place, but for me to trust and consider the results of a study valid, I really have to go through it with a fine tooth comb, and make sure it’s a completely altruistic study, and there were no flaws in the study that I can see. I just have found it much more efficacious to observe the real world results/ experiences that people are having
A good example, imo, is all the studies that show negative issues from nandrolone monotherapy at low dosages. If testosterone didn’t convert to E2 at the rate that it does, it would be neurotoxic. E2 is what prevents test from being neurotoxic. So slight differences can make a huge impact on how we view a compound, and the effects it can potentially have. Most guys that use nandrolone for hrt purposes are taking it while having decent E2 levels. Until they do studies using nandrolone while making sure the man’s E2 is in a healthy range, I put very little weight in nandrolone monotherapy studies, at low dosages, in regards to its supposed negative effects on the heart, compared to testosterone.
Last edited:
My Prolactin is a bit high at 448 and the UK range is 86-324 mU/L. One doc said to me its not a problem another said I should take Cabergoline to lower it at 0.25mg twice a week. I wondered what is the benefit to lowering it to what level for us on TRT. I was told its normal to have high Prolactin on TRT?. Do we feel any better if it is lower, I did read that high Prolactin can increase fat round the middle, I must say I find it hard to shift the love handles , whether we can blame that on Prolactin I dont know and how high does it have to be to cause fat. I also wonder if it someway interferes with the efficiency of T etc. In other words whats wrong with having slightly elevated Prolactin.?
The dose of cabergoline (Dostinex®) you cite above is quite reasonable. Most men on TRT (testosterone replacement therapy) will have an increase in prolactin unless they are monitored for estrogen increase that is routinely related to aromatization of T to estradiol. It is called aromatization because the enzyme is an aromatase. Therefore, for men on TRT, I also advise a low dose of either anastrozole (Arimidex®) or exemestane (Aromasin®) and I check to ensure the estradiol (E2) is within normal limits. I have not seen any adverse side-effects (AES) when using such low dose cabergoline, and very rarely does any patient complain about side effects from the aromatase inhibitor. Of course, and most importantly, men on TRT should monitor PSA. I have had a half dozen patients develop prostate cancer while on TRT with two having evidence of metastatic disease from prostate to bone.
Be careful when messing with Cabergoline. It can crash your prolactin and has negative effects on dopamine in the long term.
I would not say that your levels are too high
I have never seen any ill effects form the use of cabergoline (Dostinex®) given at doses of 0.25 mg biw or tiw (twice or three times a week). Many of my patients are on this regimen for years. One thing I do note that if you are on cabergoline for many months, often you can stop it and still see prolactin suppression that lasts for months. There is no commercial lab that I know of that measures dopamine, so the best I can do is assume that if I suppress prolactin. then I am encouraging higher levels of dopamine.
Bromocriptine is not an easy drug with nausea and vomiting a major side effect. This is in stark contrast to cabergoline that is very patient friendly. I was an investigator for cabergoline with the pharmaceutical company that eventually got FDA approval. I am pissed that this drug is absurdly priced and given it has been around for at least 20 years it should have generic product(s) available.okay thats interesting, were you on 0.25 once or twice a week,I wonder if maybe 0.25 a fortnight might work, will look in to Bromo, any idea on dosing etc
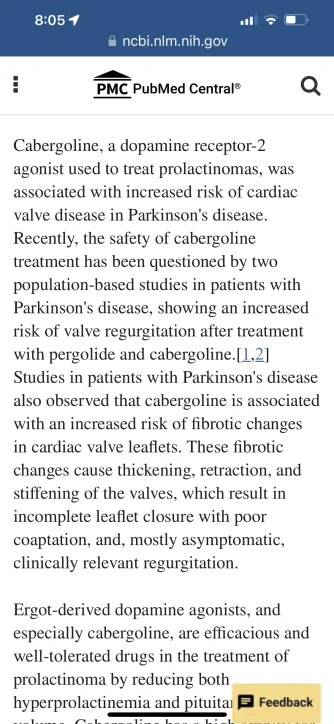
Not trying to be sarcastic or anything like that. I’m genuinely curious since u were an investigator for the company that eventually got fda approval to sell cabergoline. Have u ever heard of cabergoline actually causing the things that pubmed is saying it does here?Bromocriptine is not an easy drug with nausea and vomiting a major side effect. This is in stark contrast to cabergoline that is very patient friendly. I was an investigator for cabergoline with the pharmaceutical company that eventually got FDA approval. I am pissed that this drug is absurdly priced and given it has been around for at least 20 years it should have generic product(s) available.
Attachments
My experience with significant lowering of prolactin using cabergoline (Dostinex®) is in a study population of older men and the vast majority were being treated for prostate cancer. This is a seriously different cohort of men than in the publication cited above. I am attaching the full paper for your interest.Sexual function and depressive symptoms in men with hypoprolactinaemia secondary to overtreatment of prolactin excess: A pilot study - PubMed
The results obtained indicate that men with dopamine agonist-induced hypoprolactinaemia are characterised by impaired sexual functioning and reduced wellbeing. These disturbances are a consequence of subnormal prolactin levels and do not seem to reflect adverse effects of dopamine agonists.
Attachments
The above is wrong. There is clear-cut evidence that TRT (testosterone replacement therapy) with high testosterone levels will stimulate E2 production via aromatase. Those high E2 levels are absolutely stimulants of prolactin. My goal as a physician is to bring happiness associated with quality of life + extension of life. I truly get euphoric when I am able to use TRT in a man who at one point in his life thought both quantity and quality of life would be cut short by prostate cancer. I only could survive the many years in medicine by having those patients I care for and about resolve their problems and regain health and happiness.There’s is no medical science backing up your doctors claim that men on TRT have high prolactin or did he learn this in medical school.
This is nonsense and is just an excuse so he doesn’t have to provide medical care.
High prolactin can cause ED.
No one has studied the effect of lowering prolactin or interfering with prolactin receptors on long term immune system function, so do not manipulate your prolactin unless you talk to your physician.My experience with significant lowering of prolactin using cabergoline (Dostinex®) is in a study population of older men and the vast majority were being treated for prostate cancer. This is a seriously different cohort of men than in the publication cited above. I am attaching the full paper for your interest.
I never received anything from the pharmaceutical company sponsoring cabergoline. In fact, a major regret in my life as an investigator for many block buster drugs was that I thought it unethical to purchase stock in these companies. If I would have done that I could have built an outstanding medical center and improved the lives of many more. The side effects you have cited below are related to much larger doses of cabergoline than the 0.25 mg twice or three times a week that I used.Not trying to be sarcastic or anything like that. I’m genuinely curious since u were an investigator for the company that eventually got fda approval to sell cabergoline. Have u ever heard of cabergoline actually causing the things that pubmed is saying it does here?
I have never seen any ill effects form the use of cabergoline (Dostinex®) given at doses of 0.25 mg biw or tiw (twice or three times a week). Many of my patients are on this regimen for years. One thing I do note that if you are on cabergoline for many months, often you can stop it and still see prolactin suppression that lasts for months. There is no commercial lab that I know of that measures dopamine, so the best I can do is assume that if I suppress prolactin. then I am encouraging higher levels of dopamine.
Low Prolactin Is Associated with Sexual Dysfunction & Psychological/Metabolic Issues - Excel Male TRT Forum
I caution men who are using cabergoline to be careful not to bring their prolactin down too low. Men use cabergoline to decrease their prolactin after a study showed that this would improve orgasms, but now a new study shows that too low of a prolactin blood level can create problems...
What I have seen working in major cities in the US and also giving presentations in Europe and Australia is that few physicians ever check prolactin levels. I would be delighted but shocked if any MD questioned could reply with evidence of knowledge about prolactin receptors or what drugs like cabergoline or bromocriptine do. The outstanding work of physician/scientists like Farnsworth and others is pretty much ignored. The importance of prolactin receptors in cancer of the prostate and breast is just about never addressed.No one has studied the effect of lowering prolactin or interfering with prolactin receptors on long term immune system function, so do not manipulate your prolactin unless you talk to your physician.
Stephen B. Strum, MD, FACP
So what are your levels prolactin and amount of cabergoline are you using?What I have seen working in major cities in the US and also giving presentations in Europe and Australia is that few physicians ever check prolactin levels. I would be delighted but shocked if any MD questioned could reply with evidence of knowledge about prolactin receptors or what drugs like cabergoline or bromocriptine do. The outstanding work of physician/scientists like Farnsworth and others is pretty much ignored. The importance of prolactin receptors in cancer of the prostate and breast is just about never addressed.
Stephen B. Strum, MD, FACP

Cabergoline is available as a generic drug, and the current price on GoodRx is less than $3 for 0.5 mg. This doesn't seem too bad considering that many on TRT need less than 0.5 mg per week to adequately reduce prolactin. When I was taking it I maxed out at 31 mcg/day. Although my symptoms somewhat improved I was still not happy with the results. My current protocol includes selegiline, which might be doing something similar.Bromocriptine is not an easy drug with nausea and vomiting a major side effect. This is in stark contrast to cabergoline that is very patient friendly. I was an investigator for cabergoline with the pharmaceutical company that eventually got FDA approval. I am pissed that this drug is absurdly priced and given it has been around for at least 20 years it should have generic product(s) available.
@Cataceous what are your levels of prolactin. And what made you get them tested?Cabergoline is available as a generic drug, and the current price on GoodRx is less than $3 for 0.5 mg. This doesn't seem too bad considering that many on TRT need less than 0.5 mg per week to adequately reduce prolactin. When I was taking it I maxed out at 31 mcg/day. Although my symptoms somewhat improved I was still not happy with the results. My current protocol includes selegiline, which might be doing something similar.
Similar threads
- Replies
- 10
- Views
- 4K
- Replies
- 6
- Views
- 6K
- Replies
- 18
- Views
- 1K

Sponsors








Online statistics
- Members online
- 2
- Guests online
- 301
- Total visitors
- 303
Totals may include hidden visitors.
Latest posts
-
Hesitating on TRT, Does Anyone Have Regrets?
- Latest: ClashCityRocker
-
-
-
 How To Inject Trimix for Erectile Dysfunction
How To Inject Trimix for Erectile Dysfunction- Latest: Nelson Vergel
-
 Effect of TRT vs hCG/FSH on upstream hormone pathways.
Effect of TRT vs hCG/FSH on upstream hormone pathways.- Latest: Fernando Almaguer