In previous studies of testicular biopsy tissue from healthy men, intratesticular testosterone (ITT) has been shown to be much higher than serum testosterone (T

academic.oup.com
Discussion
A significant intratesticular fluid to serum T gradient was observed in this group of young normal men at baseline. In this study, serum T was 1.2% of ITT, an 84-fold gradient. A similar testicular to serum gradient has been reported in studies of testicular biopsy tissue in the 1970s (19) as well as more recently (9, 13). However, the absolute ITT levels reported in testicular homogenates are higher than the ITT levels found in the testicular fluid aspirates in this study. This difference is probably the result of the release of cellular T stores in testicular homogenates compared with secreted T in fluid aspirates obtained with minimal cellular disruption.
Normal intratesticular fluid T concentrations were maintained by low doses of hCG (125, 250, and 500 IU every other day for 3 wk) in men with gonadotropin suppression from exogenous T. Presumably, normal ITT levels within the testis should support normal spermatogenesis.
madman, thank you for posting these studies. it stated in one '
Furthermore, we have demonstrated that very low-level LH-like stimulation of the testes with hCG increases IT-T in a dose-dependent manner. Importantly, our results suggest that the threshold dose for stimulating IT-T in humans is likely to lie between 15 and 60 IU of hCG.
does this also hold true for men doing trt with hcg? They stated that they thought men using hcg alone where more responsive to it, just wondering if trt further reduced responsiveness hence high dose hcg needed for them?
As expected, we observed that serum gonadotropin levels were significantly reduced by exogenous T in this study. Gonadotropin suppression without hCG administration caused dramatic reductions in ITT (94%) from baseline in the TE and placebo hCG group. Exogenous TE (200 mg weekly) has also been shown to reduce sperm production to azoospermic levels in approximately 70% of Caucasian men (7, 8). Spermatogenesis was not assessed in this 3-wk study, but in a previous study of normal men (n 7) with gonadotropin suppression induced with 6 months of T and a progestin, levonorgestrel (LNG), intratesticular fluid T was suppressed 98% from baseline (15).
In this study, hCG increased the ITT concentration, presumably through stimulation of Leydig cell steroidogenesis. The dose of hCG required to maintain baseline ITT concentrations in men with maximal gonadotropin suppression is significantly lower than that historically used in the treatment of infertility due to hypogonadotropic hypogonadism.
A review of the literature reveals a broad range of relatively high doses of gonadotropin replacement using hCG ranging from 1250 IU three times weekly to 3000 IU twice weekly (29 –32). Even higher doses of hCG (5000 IU, three times per week) have been shown to be safe in experimental models of gonadotropin withdrawal (33, 34). Regimens of 2000 IU administered im two or three times weekly have been used with hCG dose adjustment according to serum T levels with a goal of normal physiological serum T levels (32, 35, 36).
This approach is based on the assumption that if normal serum T levels were established by hCG administration, ITT concentrations would be sufficient to support normal spermatogenesis. However, ITT was never directly assessed in these studies. The minimum hCG dose needed to restore ITT to levels sufficient for initiating and maintaining spermatogenesis is not known.
All three hCG groups in this study (125, 250, and 500 IU, given every other day) maintained ITT at levels statistically indistinguishable from the baseline. These doses are 10–20% of the doses commonly used in male infertility treatment (1250–2000 IU, two or three times weekly). Endocrinologists and andrologists have been aware that the doses of hCG traditionally used to treat certain types of infertility are supraphysiological and may expose patients to high levels of T and estradiol, with the consequent risk of clinically significant gynecomastia (37). The ability to prescribe hCG doses at lower levels to target normal serum and ITT and normal spermatogenesis would be useful for this patient population.
However, men rendered hypogonadotropic with exogenous T administration are different from men with infertility due to hypogonadotropic hypogonadism in two important ways. First, the study participants started with normal gonadotropin levels and were treated with high dose TE to induce gonadotropin withdrawal at the same time they were treated with hCG with the aim of maintaining ITT. In contrast, hypogonadotropic infertile men are treated with either T replacement or hCG for fertility, but not both simultaneously. The weekly administration of TE raised serum T levels significantly in all groups and may have resulted in higher ITT concentrations than would have been observed in a patient with hypogonadotropic hypogonadism receiving hCG therapy alone. Second, in the clinical setting, ITT production and spermatogenesis have to be induced after a prolonged period of gonadotropin deficiency. Therefore, the low-dose hCG used in this study may not normalize ITT in hypogonadotropic infertile men. However, lower hCG doses than those traditionally used may be sufficient to restore spermatogenesis.
In summary, assessment of the testicular hormonal environment through percutaneous fluid aspiration has shown a similar testis to serum T gradient as previous testicular biopsy studies in men and rats. Additionally, low doses of hCG maintain baseline levels of ITT in men with gonadotropin withdrawal from exogenous T administration. Lower doses of hCG may be as effective in treating male infertility due to hypogonadotropism as the higher doses used historically. Selective replacement of LH activity with low-dose hCG, as demonstrated in this study, will allow the design of future studies investigating the relative roles of intratesticular androgens and FSH in the control of human spermatogenesis. Such work will be applicable to the goal of developing uniformly effective male contraception.
Context and Objective: In men with infertility secondary to gonadotropin deficiency, treatment with relatively high dosages of human chorionic gonadotropin

academic.oup.com
Discussion
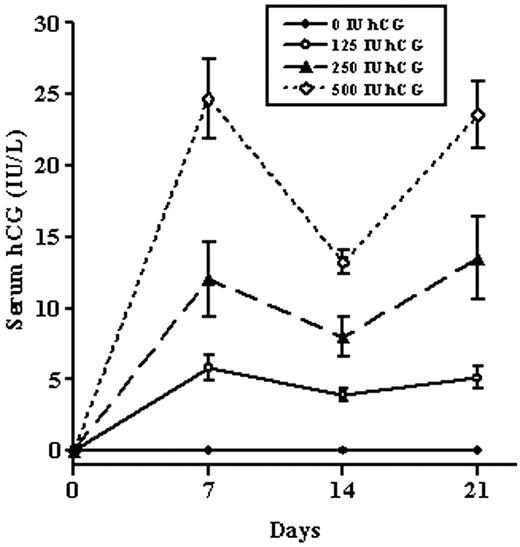
In the study, we used testicular aspiration, coupled with gonadotropin suppression, and graded, low doses of hCG to determine the dose-response relationship between intratesticular androgens and hCG in man. This study is the first to examine the relationship of such low doses of hCG with intratesticular androgens and to correlate the concentrations of intratesticular androgens with contemporaneously measured serum hormones. Interestingly, we have shown that IT-T concentrations remain much higher than serum testosterone concentrations despite marked LH suppression. Furthermore, we have demonstrated that very low-level LH-like stimulation of the testes with hCG increases IT-T in a dose-dependent manner. Importantly, our results suggest that the threshold dose for stimulating IT-T in humans is likely to lie between 15 and 60 IU of hCG. The measurement of IT-T, coupled with sensitive and specific liquid chromatography-tandem mass spectrometry hormone measurements, and longer-term low-dose gonadotropin administration in this experimental gonadotropin-deficient human model will permit more detailed investigation of the hormonal regulation of spermatogenesis in man than previously possible.
Normal men appear to be more sensitive to hCG than infertile men with hypogonadotropic hypogonadism. This difference in sensitivity is likely due to the fact that steroidogenesis in men with long-term gonadotropin deficiency is impaired, possibly secondary to Leydig cell immaturity. A similar phenomenon has been observed in the hpg mouse, in which larger doses of gonadotropins are required to initiate spermatogenesis than to maintain it once established (19).
Our previous work in this area, which used doses of hCG closer to those used in hypogonadotropic infertile men, resulted in IT-T concentrations that were not significantly lower than normal (15). Therefore, in this study, we chose very low doses of hCG to better understand the full dose-response relationship. Notably, in this study, we found that having normal serum testosterone while receiving hCG does not correspond to an IT-T concentration similar to those observed at baseline. The implications of this for the induction of spermatogenesis in men with hypogonadotropic hypogonadism are unknown. However, it is possible that the observation that serum hCG is highly correlated with IT-T may prove useful in the treatment of men with infertility from gonadotropin deficiency. As a result, clinicians may consider measuring both serum testosterone and serum hCG to ensure the adequacy of treatment; however, future studies of the relationship between serum hCG and IT-T in men with hypogonadotropic hypogonadism will be required to determine the utility of this measurement.
In conclusion, this study demonstrates the strong dose-response relationship between IT-T and very low-dose hCG administration in gonadotropin-suppressed men. This work provides crucial information for future studies determining the role of intratesticular androgens on spermatogenesis in men and may improve the treatment of men with infertility and inform efforts to develop male hormonal contraceptives.