@madman
My follow-up with my provider today went well. We are going to
lower my dosage from 200mg/week to 180/week; switch from 2X/week injections to 3X/week; and aim to lower estrogen by increasing Danazol dosage. Further, I need to continue monitoring T3 and increase my caloric consumption.
He wasn’t overly concerned about the high numbers.
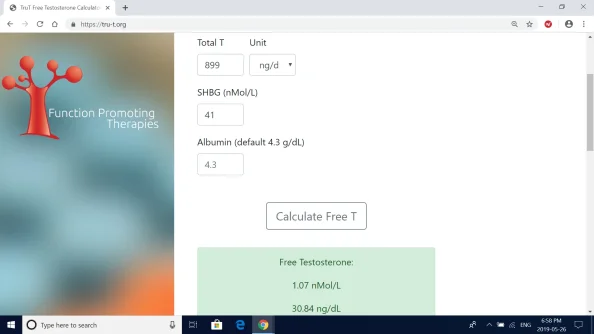
Right now, my Free T is 54.3 (using the decimal-point conversion system), and we are hoping to see it around 40 next time around. We are also hoping to see SHBG go down more and E go down.
Our meeting largely focused on estrogen. He says our goal is to get the E number to be lower than the SHBG number.
He gave me the flexibility to decide how much to increase my Danazol dosage and was happy to go up to 25 mg ED (previously: 25 mg EOD). I’m hoping for some insight here. I was thinking I would do 25 mg 5X/week.
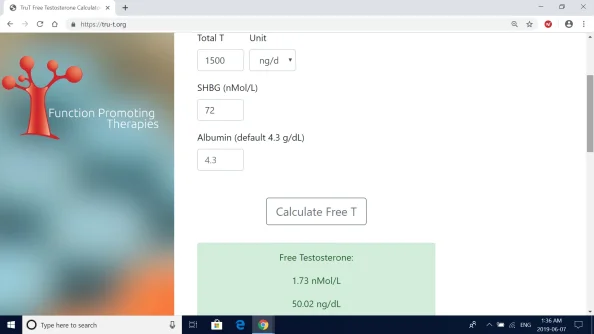
My goal is to get SHBG under 50 (was 72 on these recent bloods after starting at 180 at the beginning of HOT). How much would you increase it? Would you go up to 25 mg ED? I do
not want to employ an AI, though I do have some on hand if needed.
It seems Danazol will intermittently be a part of my protocol for the foreseeable future.
Once we get SHBG sufficiently low — which will allow me to have a more moderate T level — we will lay off the Danazol for a while, then reintroduce it if SHBG increases too much. This cycling system will be in place to reduce the risk of liver toxicity. That liver toxicity possibility is why I'm not ruling out an AI entirely. It may need to come into play at some point.
We also talked a lot about my high Reverse T3. He believes this is a result eating too few calories — something he sees a lot in
bodybuilders who do caloric restriction. He believes I should be eating a lot more (currently: all the way down to 1800 cals, as I have been cutting for 2 months). My T3 is now 9% of my Reverse T3, and our goal is for it to be 20% or more. But raising thyroid hormones can also raise SHBG, so we are going to leave this alone for now and just roll with the other changes I outlined above. We’ll continue monitoring.
I plan to increase my food consumption -- how much do you think I should be eating? I am 6'2", 175 lbs., and rather active (lift 6 days a week, cardio 2 days, 10K+ steps every day). He recommended 3500/day, but that seems like an extreme leap to me.
Final note:
he didn’t think I necessarily needed more bloodwork now (as opposed to in 6 weeks), but I asked for it. Thus, I will have a CBC and CMP now. As I understand it, these tests should comprise HCT, HGB, and RBC, among other variables.
He wasn’t super concerned about HCT because my level has been quite stable throughout treatment on the four tests I’ve had (45, 46.6, 44, 45.7). But it will be interesting to see how much it has jumped up, given the rise in Free T.





.webp")