

BadassBlues
Well-Known Member
Although some consistency has been established with regard to Sirolimus protocols and dosing, there still remains some unanswered questions. My questions are specific to those of us who are either bodybuilders, athletes or fitness enthusiasts that don't necessarily wish to suppress protein synthesis for extended periods of time. I am currently on 5mg biweekly and am considering a bump in the dosage to 6mg but intend to maintain the biweekly schedule.
Many of the clinics and doctors prescribing Sirolimus use the weight of the patient as a dosage regulator. Doses up to 10 mg are prescribed, mostly on a weekly protocol. With the half-life being 60-80 hours, this seems excessive to me for the subset mentioned above. There hasn't been any real reporting of these doses affecting Mtor2, but that seems like a major suppression of protein synthesis.
Perhaps @Nelson Vergel could inform us if Discount Labs offers a Sirolimus test? Life Extension has one for 99.00. This could be used to check peak levels after 2-3 hours and trough after 60-80 hours.
Also, dosage timing is more important than originally considered. Morning doses on an empty stomach 2-3 hours before eating is recommended as fats can have an effect on efficacy.

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
Here is some useful information:
 www.rapamycin.news
www.rapamycin.news
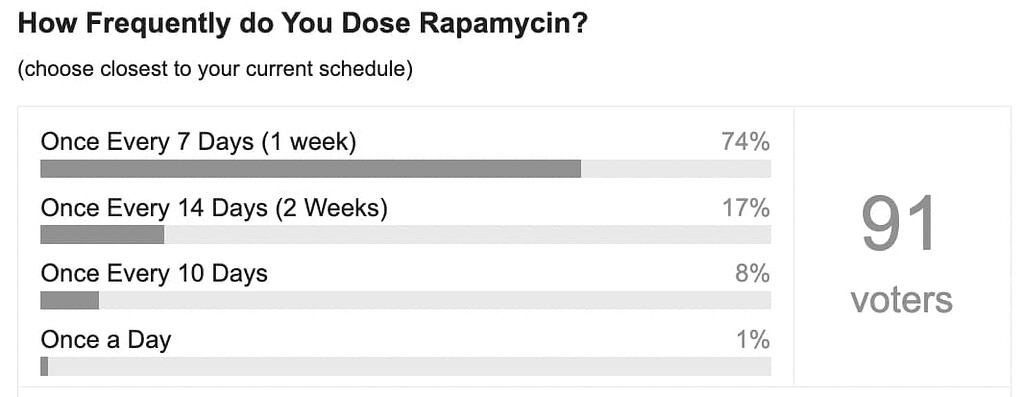
Here are the common dosing variables that I see people considering when they start dosing rapamycin for anti-aging (from an August, 2022 user poll 49 here on our site):

RapadosingFreq1066×414 26.3 KB
RapaDosingLevel1070×1304 61.9 KB
Note: Most users taking rapamycin for anti-aging, take between 3mg and 10mg per week, on a once-weekly dosing schedule. Our forum software doesn’t accommodate conditional branching in these surveys, but most of the doses above 10mg are likely people who are dosing once every 10 days or 2 weeks, so an effective weekly dose of between 5 and 10mg per week. A few people are trying much higher dosing levels.
1. Starting Dose and Ramping Up the Dose:
I started at 1mg per week, then each week increased by 1mg until I reached my target dose of 6mg/week. Most people, working with their doctor, seem to end up taking between 3mg and 10mg of rapamycin in a single weekly dose. (see recent poll results above)
In my case, many months after I plateaued at 6m per week, I slowly increased to my current dose of 10mg/week. This has worked well for me, with only one time when I got a canker sore (which cleared up by itself after a few days). Other people ramp up more quickly - for example 3mg/week, then 6 mg a week… Generally I seem to see more side effects the faster the ramp up in dose.
Patient’s of Dr Green say he recommends taking rapamycin in the morning as it can be stimulative.
Patient’s of Dr. Green have conveyed that he has the following blood tests ordered before the initial visit, to get a baseline of information:
See more details here: Impressive Biological Age Reductions with Rapamycin (anecdotal)
People also say Dr. Green also strongly recommends people get their DNA sequenced (e.g. 23andMe), primarily to look for the APOE variants which are suggestive of increased risk for Alzheimers.
Other people look at additional blood tests for additional information:
A consideration for what food to take with/before taking the rapamycin: How to Improve Bioavailability, Lower the Cost, of Rapamycin
2. Timing of the Dose (weekly, every two weeks, etc.)
Most people taking rapamycin for anti-aging seem to have settled on a weekly dose, largely because that was the dosing frequency originally used in the Mannick 2014 Study of the rapalog everolimus 321. That study used a weekly dose and saw only minor side effects over the period of the study.
Other people are looking at the research on the half-life of rapamycin (typically cited as somewhere between 62 and 80+ hours - and seems to vary by age and ethnicity) and then evaluating their dose and weight and determining when their blood sirolimus levels are at a trough level that they consider safe enough for the next dose. For some people this is 10 or 12 days. As you can see in the graph below tracking blood sirolimus levels over time, there is a quick initial peak about 1 hour after taking the medicine, and then it decreases by about 50% every 65 to 85 hours (source 41).
Recently the Life Extension Foundation Lab services 83 has started offering a low cost blood test for blood sirolimus levels 120 via Labcorp. testing services. They sent this email to me recently:
This may be a good way to make sure your dosing schedule is working in terms of minimizing risk of MTORC2 inhibition.
Screen Shot 2021-10-06 at 10.49.26 PM952×1178 100 KB
Lately, some people have started taking higher doses (e.g. 20mg) with a once every two weeks dosing schedule. This has been adopted by Dr. Mikhail Blagosklonny because he believes that the higher intial dose may help penetrate the blood brain barrier (see tweet here 111).
Blag20mg994×952 56.2 KB
On Twitter, Aging-focused Doctor 155 has mentioned a patient who is using 20mg rapamycin every week: (sources here 33 and here 14)
We don’t yet know what the optimal doses, or dosing schedules, are for anti-aging, but the current theory that many of the rapamycin researchers think may be true is that the higher the dose, (and more frequent the dose) and the longer the use of rapamycin, the greater the risk of potentially blocking the MTORC2 pathway, which can lead to reduced immune system function and risk of increased infections and other issues. We have not see this issue much at all in this user group, on the weekly or every two week dosing schedules. Given the lack of any issues related to immune function that we’ve seen, most people today do not do “rapamycin vacations”, but some still do. So, to make sure they are not blocking MTORC2 some people are taking periodic “vacations” from rapamycin (of a few weeks or longer), so as to be sure that the MTORC2 pathway is not excessively inhibited, and is allowed to return to normal function.
There is no research yet on the details of how much time is the right amount of time-off from rapamycin to allow this, so its all guess work right now.
In Peter Attia’s podcast interview with Joan Mannick and Nir Barzelai 348 he mentioned his dosing protocol and the rationale behind it:
Many of the clinics and doctors prescribing Sirolimus use the weight of the patient as a dosage regulator. Doses up to 10 mg are prescribed, mostly on a weekly protocol. With the half-life being 60-80 hours, this seems excessive to me for the subset mentioned above. There hasn't been any real reporting of these doses affecting Mtor2, but that seems like a major suppression of protein synthesis.
Perhaps @Nelson Vergel could inform us if Discount Labs offers a Sirolimus test? Life Extension has one for 99.00. This could be used to check peak levels after 2-3 hours and trough after 60-80 hours.
Also, dosage timing is more important than originally considered. Morning doses on an empty stomach 2-3 hours before eating is recommended as fats can have an effect on efficacy.
The effect of a high-fat meal on the oral bioavailability of the immunosuppressant sirolimus (rapamycin) - PubMed
The bioavailability of an oral nonaqueous solution of sirolimus was compared under fasting conditions and after a high-fat meal in a randomized, two-way crossover pharmacokinetic study. Healthy volunteers were administered a 15 mg single dose of sirolimus on two occasions, once while fasting and...
pubmed.ncbi.nlm.nih.gov
Here is some useful information:
What is the Rapamycin Dose / Dosage for Anti-Aging or Longevity?
Rapamycin Dosing Level and Timing Here are the common dosing variables that I see people considering when they start dosing rapamycin for anti-aging (from an August, 2022 user poll here on our site): Note: Most users taking rapamycin for anti-aging, take between 3mg and 10mg per week, on...
www.rapamycin.news
Here are the common dosing variables that I see people considering when they start dosing rapamycin for anti-aging (from an August, 2022 user poll 49 here on our site):

RapadosingFreq1066×414 26.3 KB

RapaDosingLevel1070×1304 61.9 KB
Note: Most users taking rapamycin for anti-aging, take between 3mg and 10mg per week, on a once-weekly dosing schedule. Our forum software doesn’t accommodate conditional branching in these surveys, but most of the doses above 10mg are likely people who are dosing once every 10 days or 2 weeks, so an effective weekly dose of between 5 and 10mg per week. A few people are trying much higher dosing levels.
1. Starting Dose and Ramping Up the Dose:
I started at 1mg per week, then each week increased by 1mg until I reached my target dose of 6mg/week. Most people, working with their doctor, seem to end up taking between 3mg and 10mg of rapamycin in a single weekly dose. (see recent poll results above)
In my case, many months after I plateaued at 6m per week, I slowly increased to my current dose of 10mg/week. This has worked well for me, with only one time when I got a canker sore (which cleared up by itself after a few days). Other people ramp up more quickly - for example 3mg/week, then 6 mg a week… Generally I seem to see more side effects the faster the ramp up in dose.
Patient’s of Dr Green say he recommends taking rapamycin in the morning as it can be stimulative.
Patient’s of Dr. Green have conveyed that he has the following blood tests ordered before the initial visit, to get a baseline of information:
- Insulin
- CBC (Complete Blood Count)
- CMP (Comprehensive Metabolic Panel
- Ferritin
- Lipid Panel
- Hemoglobin A1C
See more details here: Impressive Biological Age Reductions with Rapamycin (anecdotal)
People also say Dr. Green also strongly recommends people get their DNA sequenced (e.g. 23andMe), primarily to look for the APOE variants which are suggestive of increased risk for Alzheimers.
Other people look at additional blood tests for additional information:
A consideration for what food to take with/before taking the rapamycin: How to Improve Bioavailability, Lower the Cost, of Rapamycin
2. Timing of the Dose (weekly, every two weeks, etc.)
Most people taking rapamycin for anti-aging seem to have settled on a weekly dose, largely because that was the dosing frequency originally used in the Mannick 2014 Study of the rapalog everolimus 321. That study used a weekly dose and saw only minor side effects over the period of the study.
Other people are looking at the research on the half-life of rapamycin (typically cited as somewhere between 62 and 80+ hours - and seems to vary by age and ethnicity) and then evaluating their dose and weight and determining when their blood sirolimus levels are at a trough level that they consider safe enough for the next dose. For some people this is 10 or 12 days. As you can see in the graph below tracking blood sirolimus levels over time, there is a quick initial peak about 1 hour after taking the medicine, and then it decreases by about 50% every 65 to 85 hours (source 41).
Recently the Life Extension Foundation Lab services 83 has started offering a low cost blood test for blood sirolimus levels 120 via Labcorp. testing services. They sent this email to me recently:
More details on $95 Sirolimus Blood test from Life Extension Corp. 188After re-evaluating current pricing for test 716712, we are able to offer it at a price of $95 going forward. Please call us if you would like to place an order. Thank you for your support and interest in our lab testing services. Life Extension Customer Support, (800) 678-8989.
This may be a good way to make sure your dosing schedule is working in terms of minimizing risk of MTORC2 inhibition.

Screen Shot 2021-10-06 at 10.49.26 PM952×1178 100 KB
Lately, some people have started taking higher doses (e.g. 20mg) with a once every two weeks dosing schedule. This has been adopted by Dr. Mikhail Blagosklonny because he believes that the higher intial dose may help penetrate the blood brain barrier (see tweet here 111).

Blag20mg994×952 56.2 KB
On Twitter, Aging-focused Doctor 155 has mentioned a patient who is using 20mg rapamycin every week: (sources here 33 and here 14)
4. Rapamycin VacationsCase report, unpublished: 20 mg rapamycin once a week (~0.36 mg/kg!) anecdotally associated with insulin<1, fasting BG in the 70s-80s, perfect lipids and other biomarkers. Cmin is below immunosuppressive transplant range, and patient doing great with subjectively better immunity despite not washing out (ie, MTORC2 feedback inhibition) between doses. ( from details posted by https://twitter.com/agingdoc1 155)
That’s no typo: 20 mg, every week. Cmax peaks/Cmin troughs to prove it. Contrary to hypothesis, BG went down rather than up (this ideal BMI subject had a bit of dawn phenomenon 29 - i.e. high morning glucose levels - that only disappeared following dose escalation to this level.
While we are addressing important issues in other model systems, what is the potential for translational work with rapamycin RCTs at such high-dose periodic regimens?
The closest thing to that is Joan Mannick’s everolimus work @ 20 mg ( and 5mg) weekly, but rapamycin is a lot more affordable, has vastly more model organism literature, and based on the clinical data we have so far (including case series in the several hundred by Dr. Alan Green, who monitors lipid panel & HOMA-IR in every patient every visit with rare material biomarker perturbations[unpublished data]) it appears very safe with the weekly dosing despite the longer half-life compared with everolimus.
I see some trials at various stages at clinicaltrials.gov 31 , esp. for Covid but only at much lower doses than the 20 mg/week ( allometric scaling and pharmacokinetics suggest doses in the 20-40mg range for humans based on the ITP results). Moreover these trials are based on either short-term or continuous dosage as opposed to long term pulsed therapy akin to work by Anisimov, & separately by Mannick (w/ raplog everolimus).
Rapamycin is serious business with real risks (& potential/theoretical benefits yet to be confirmed), so less anarchy and the cultivation of more systematic approaches - carefully weighing risks versus benefits as clinically appropriate to that situation - would be a good thing…
We don’t yet know what the optimal doses, or dosing schedules, are for anti-aging, but the current theory that many of the rapamycin researchers think may be true is that the higher the dose, (and more frequent the dose) and the longer the use of rapamycin, the greater the risk of potentially blocking the MTORC2 pathway, which can lead to reduced immune system function and risk of increased infections and other issues. We have not see this issue much at all in this user group, on the weekly or every two week dosing schedules. Given the lack of any issues related to immune function that we’ve seen, most people today do not do “rapamycin vacations”, but some still do. So, to make sure they are not blocking MTORC2 some people are taking periodic “vacations” from rapamycin (of a few weeks or longer), so as to be sure that the MTORC2 pathway is not excessively inhibited, and is allowed to return to normal function.
There is no research yet on the details of how much time is the right amount of time-off from rapamycin to allow this, so its all guess work right now.
In Peter Attia’s podcast interview with Joan Mannick and Nir Barzelai 348 he mentioned his dosing protocol and the rationale behind it:
- Joan’s paper 321 suggested 5 mg once a week was a pretty good place to start
- Peter triangulated that data with data from Matt Kaeberlein’s dogs 125
- He settled on 6 mg once a week
- What still remains unclear for Peter is how to cycle it
- Current protocol is—on for 8 weeks, off for 5 weeks
- “But, truthfully, without more advanced testing, I’m really making it up and therefore I don’t like talking about it like I just did .”











