Your doctor not wanting to talk about your testosterone panel, huge red flag!
Your doctor is using the Direct FT method, often inaccurate and overestimating FT results, the equilibrium dialysis method being the most accurate method or even the calculated method.
If your doctor had tested SHBG, we could then calculate your FT using your Total T and SHBG using ->
FT calculator to verify if your FT result is accurate. Men with low TT will have lower SHBG, as SHBG is a function of SHBG.
There's no point in waiting 6-8 weeks, no reason why you can't retest in a few days to a week.
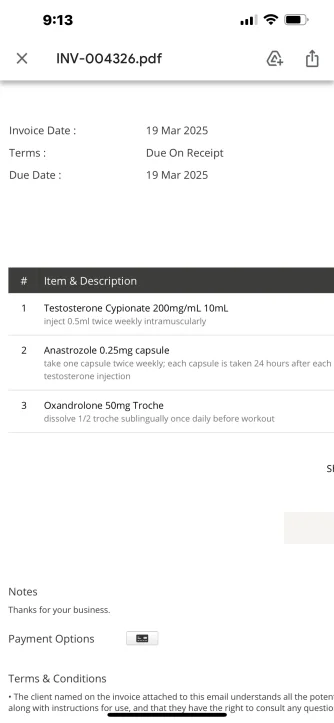
In our healthcare system you may have many hurdles to overcome to get a proper diagnosis and treatment through insurance based healthcare. For these folks, using private cash pay clinicals for TRT is another option.
Something you should know, low-T is a disease that always accompanies another medical problem and while TRT can give you to opportunity to correct your health, for some, for awhile TRT brings about many benefits if only temporarily, as the main cause of the low-T is left untreated.
It's advisable to find out the cause of your low-T.
How's your sleep? This is a big influence on testosterone production! I do have sleep apnea
Describe your diet. Also, if eating processed foods, the western diet, creating western diseases, the leading cause of health problems worldwide. Actually pretty clean, high protein, reduction focus on cards and very very little sugar
Getting in a state of ketosis, like the carnivore diet has the potential to cure many diseases/health problems. Your doctor doesn't know this, because nutrition education is lacking in medical school and many doctors are dishing out wrong dietary information.
Do you exercise? Same here, lack of exercise, a body at rest tends to stay at rest and soon this becomes the normality for your body as you develop metabolic disorders. Low SHBG is strongly associated with metabolic disorders. This can be increased most definitely
You're missing
thyroid labs, checking TSH, fT3 and fT4. A thyroid problem can lead to low SHBG. I had a full work up 3 month ago, all that was good to go across the board