T
tareload
Guest
View attachment 7259
[0026] Fig. 7 depicts the thermodynamic Parameters associated with testosterone's binding to SHBG derived from the fit of binding isotherms and ITC data to new model. While this parameter set is not unique, together they consistently describe the binding isotherms, depletion curves and ITC data to the new Multi-step Dynamic Binding Model with Complex Allostery developed in this study. These were utilized to obtain FT values (cFTZBJ) in samples obtained in clinical trials.
View attachment 7260
[0027] Figs. 8A-8B demonstrate that the binding of testosterone to SHBG displays complex allostery. Fig. 8A depicts a graph demonstrating that binding isotherms display significant non-linearity. Varying concentrations of testosterone were incubated with a fixed concentration of SHBG (5, 10 or 20 nM) and bound testosterone was plotted against total testosterone concentration. The binding isotherms were generated at 5, 10 and 20 nM SHBG. Curves represent the result of the fit of data to the new Multi-step Dynamic Binding Model with Complex Allostery.
View attachment 7261
Fig. 8B depicts a graph demonstrating that depletion of FT by varying SHBG concentration is best described by the new Multi-step Dynamic Binding Model with Complex Allostery. Constant concentration of testosterone (6, 12 , 17 or 32 nM) was incubated with increasing SHBG concentrations, and free testosterone concentration in buffer side was plotted against SHBG concentration. The curves are the result of the fit of data to the new Multi-step Dynamic Binding Model with Complex Allostery.
View attachment 7262
[0028] Figs. 9A-9C depicts graphs depicting the fits of the various models of testosterone's binding to SHBG to the experimental data from binding isotherms, depletion experiments, and ITC. Left panels: The figures show the fits of data to the various models examined in this study.Right panels: The figures show corresponding residuals of the fit of data to various models of testosterone's binding to SHBG. Neither the Vermeulen's equation nor the simple allostery models adequately fit the experimental data from binding isotherms, depletion experiments, or ITC. The new Multi-step Dynamic Binding Model with Complex Allostery (model E) provided the optimal fit to the experimental data from all three methods.
View attachment 7263
[0029] Fig. 10 depicts a schematic of the control of testosterone levels.
View attachment 7264
[0030] Fig. 11 depicts a schematic of an exemplary system of determining free testosterone levels and/or dosages.
View attachment 7265
[0031] Fig. 12 depicts a device or a computer system 1000 comprising one or more processors 1300 and a memory 1500 storing one or more programs 1600 for execution by the one or more processors 1300.
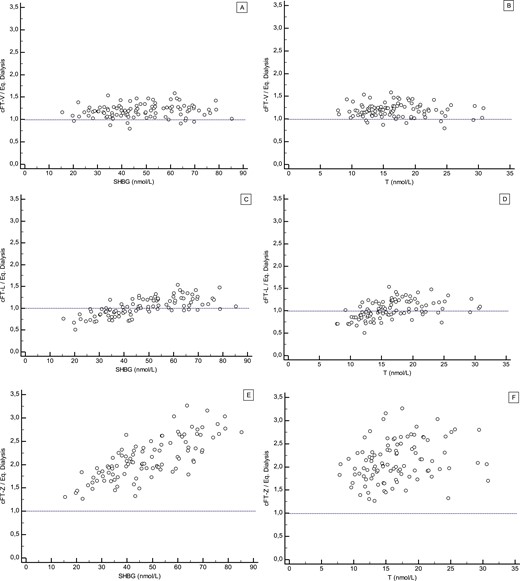
It would be an interesting plot to pool all the published data over last 10 years for equilibrium dialysis data points and then also plot Vermeulen and Tru-T on same plot. You could plot against total T or SHBG. Unless I am missing something you are going to get a cluster of data points that are very close to Vermeulen and a country mile away from Tru-T. Then another cluster that sit on top of Tru-T line. What does that say about the agreement between the various equilibrium dialysis measurement data between labs in the papers?
I conclude that if you had access to all those blood samples and ran head to head equilibrium dialysis tests you will get very different numbers. My apologies if I missed this discussion some where else. Something ain’t right with the interlab agreement on the equilibrium dialysis data.