It turns out I had crazy high blood pressure (170/100), likely for months, too much caffeine, stress and I'm 125kg/275 pounds / 192cm/6'4, 44 years old.
Last week a cardiologist put me on Dipperam 5+160 (5mg Amlodipine + 160mg Valsartan), using this first once a day and after 2 days moved on to twice a day, which puts me around 127/78 after 1 week.
The maximum effect comes around 3-4 weeks, so I should soon be at 120 or below with that.
The cardiologist also sent me to have a ultrasound heart analysis by another doc, who found my heart Ejection Factor is only 48% (normal: 50-70) and I have some left ventricle hypertrophy (38mm). The doc commented that for my age (44 years old), 48% is way too low and this must be looked at.
I have been reading a lot on the topic and came to the conclusion that Nebivolol might be the best option to help with Ejection Factor, in general, this seems the beta blocker with the least negative side effects and potential positives (increase in NO, antioxidant profile, reduction of glucose, reduction of heart rate, etc.), a 10% increase seems likely with only 3 months at 5mg / day, and the left ventricle hypertrophy may also be reversed:
after 3 months of orally administered nebivolol (2.5 and 5 mg, n = 6)
[...]
Left ventricular function increased (ejection fraction 31.5 +/- 10.11 to 42.0 +/- 10.99%, P < or = 0.01) after 12 weeks of nebivolol. The left ventricular end-systolic diameter decreased in the nebivolol-group from 56.5 +/- 9.40 to 50.2 +/- 9.43 mm (P < or = 0.02).
From: Effect of nebivolol on left ventricular function in patients with chronic heart failure: a pilot study - PubMed
I also found this YouTube Video really interesting:
Questions:
Other clarifications for additional background:
Some life style notes: no coffee or caffeine in the last 2 weeks (lots of this before), magnesium: 500mg @ morning + 700mg @ night, citrulline malate here & there, trying to do hot baths (1h x 3 times / week after weight training) due to no sauna, 45min static bike x3 times a week, weight lifting 3 days / week.
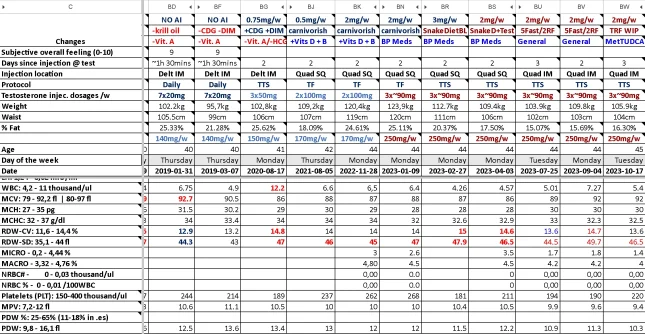
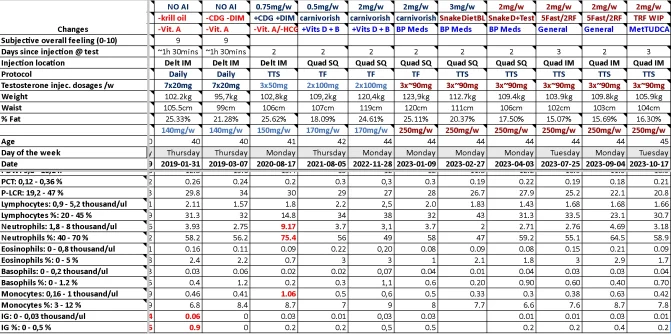
My TRT protocol:
200mg weekly (real dose ~170mg or less due to ampule extraction, loss in injections, etc.)
2 injections: MF, 100mg each (likely ~80-90 max)
hCG in the same injection
Anastrozole 2mg / week, 1mg on injection day (This would be high for most people but seems to work well for me, otherwise my E2 goes too high)
Daily cialis: 10mg, now testing 5mg morning + 5mg evening
Common supplements: Creatine, Pregnenolone, DHEA, Boron, Vitamin D3+K2, desiccated beef organs
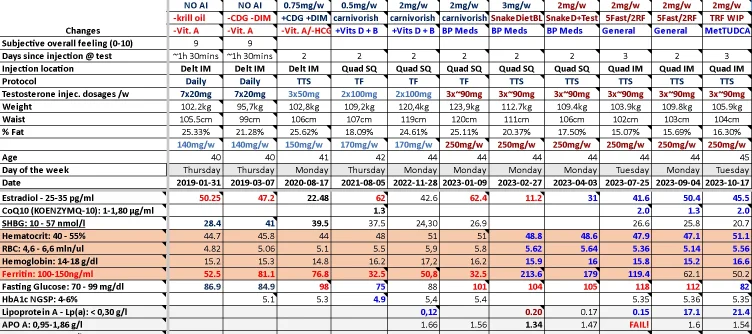
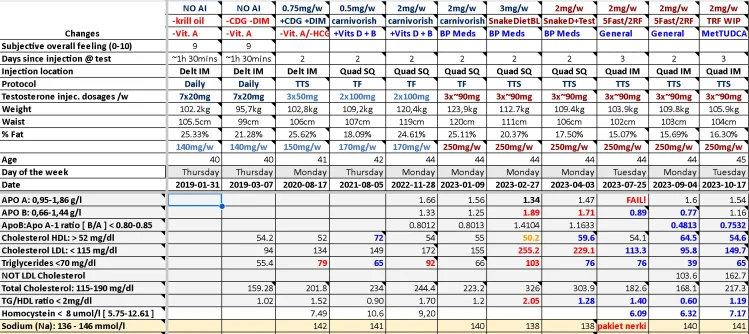
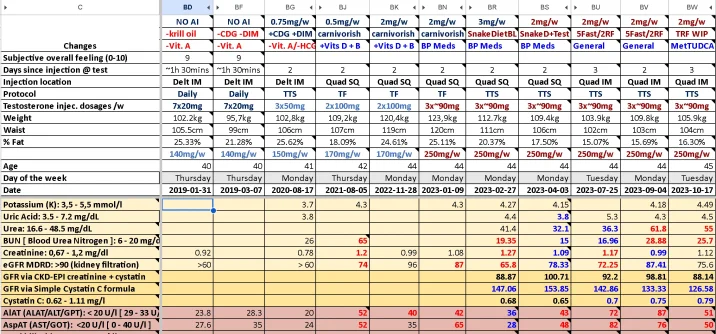
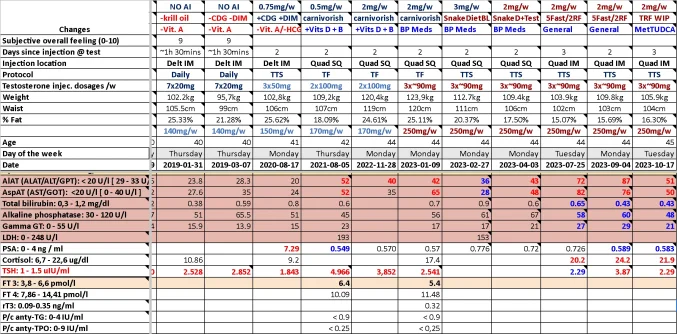
Recent labs:
Total T: 967.9
Free T: 32.41
E2: 42.6
Ferritin: 50ng/ml
Last week a cardiologist put me on Dipperam 5+160 (5mg Amlodipine + 160mg Valsartan), using this first once a day and after 2 days moved on to twice a day, which puts me around 127/78 after 1 week.
The maximum effect comes around 3-4 weeks, so I should soon be at 120 or below with that.
The cardiologist also sent me to have a ultrasound heart analysis by another doc, who found my heart Ejection Factor is only 48% (normal: 50-70) and I have some left ventricle hypertrophy (38mm). The doc commented that for my age (44 years old), 48% is way too low and this must be looked at.
I have been reading a lot on the topic and came to the conclusion that Nebivolol might be the best option to help with Ejection Factor, in general, this seems the beta blocker with the least negative side effects and potential positives (increase in NO, antioxidant profile, reduction of glucose, reduction of heart rate, etc.), a 10% increase seems likely with only 3 months at 5mg / day, and the left ventricle hypertrophy may also be reversed:
after 3 months of orally administered nebivolol (2.5 and 5 mg, n = 6)
[...]
Left ventricular function increased (ejection fraction 31.5 +/- 10.11 to 42.0 +/- 10.99%, P < or = 0.01) after 12 weeks of nebivolol. The left ventricular end-systolic diameter decreased in the nebivolol-group from 56.5 +/- 9.40 to 50.2 +/- 9.43 mm (P < or = 0.02).
From: Effect of nebivolol on left ventricular function in patients with chronic heart failure: a pilot study - PubMed
I also found this YouTube Video really interesting:
Coach Steve's Experience with Nebivolol; Heart Rate, Blood Pressure & Fat Loss. Vigorous PEDs
Questions:
- Is Nebivolol one of the best options to [ improve Ejection Factor + reduce left ventricle hypertrophy ] OR is there something better with low potential for negative side effects?
- Should I just add Nebivolol to the already working "5mg Amlodipine + 160mg Valsartan" combo, or should I try to get rid of Amlodipine if blood pressure starts to go too low?
- Depending on blood pressure numbers, would Nebivolol + Telmisartan be a good option once I lose some fat? (10kg/20lbs should result in a ~20 point blood pressure reduction in my case, but this will take at least 3 months, trying to minimize muscle loss)
- Would Doxazosin be comparable to Nebivolol to improve Ejection Factor & reduce left ventricle hypertrophy?
Other clarifications for additional background:
Some life style notes: no coffee or caffeine in the last 2 weeks (lots of this before), magnesium: 500mg @ morning + 700mg @ night, citrulline malate here & there, trying to do hot baths (1h x 3 times / week after weight training) due to no sauna, 45min static bike x3 times a week, weight lifting 3 days / week.
My TRT protocol:
200mg weekly (real dose ~170mg or less due to ampule extraction, loss in injections, etc.)
2 injections: MF, 100mg each (likely ~80-90 max)
hCG in the same injection
Anastrozole 2mg / week, 1mg on injection day (This would be high for most people but seems to work well for me, otherwise my E2 goes too high)
Daily cialis: 10mg, now testing 5mg morning + 5mg evening
Common supplements: Creatine, Pregnenolone, DHEA, Boron, Vitamin D3+K2, desiccated beef organs
Recent labs:
Total T: 967.9
Free T: 32.41
E2: 42.6
Ferritin: 50ng/ml





")

")