LH and FSH are always normal. SHBG is high, so testosterone is normal on lab tests. DHEA is low, IGF is normal(180)
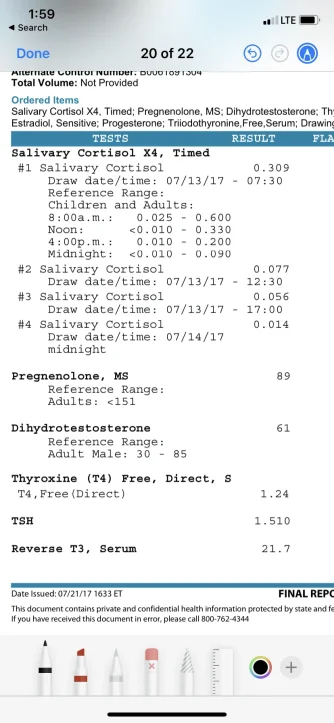
Dr Saya analyzed my cortisol
-Said morning was half of what it should be
-Said by noon it dropped really low
-Said evening was almost zero
No medicine besides DHEA/pregnenalone pills
I have never heard anything besides ACTH stimulation. It seems impossible to even find an endocrinologist that has any experience or knowledge to do what you recommended. And I’ve seen 4 of them.