Even then we need to wait on harmonized FT reference ranges based on a standardized FT assay (ED-LC/MS/MS).
Similar to what was done for harmonized TT.
*Assays that are standardized are designed to provide accurate results, traceable to “true” value-assigned certified reference materials and gold-standard reference methods.
The CDC has been working hard on this and it is not too far off now!
Soon enough we will have a CDC Hormone Standardization Program (CDC HoSt) Certified Free Testosterone Procedure and a harmonized reference range for free testosterone!

www.excelmale.com
View attachment 43656
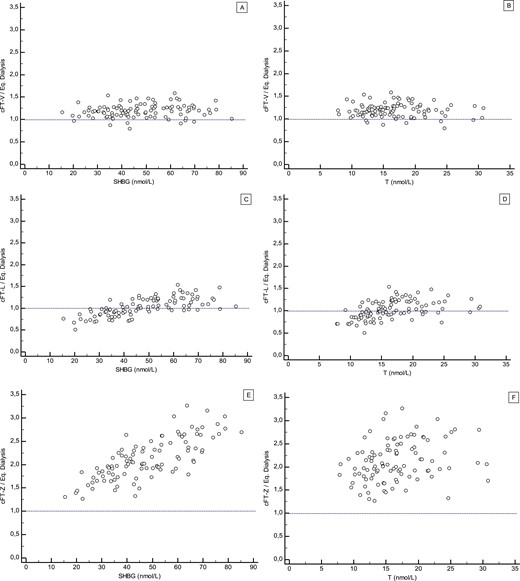
Something to keep in mind when it comes to using/relying upon the calculated FT methods!
*Currently, the CDC is developing a harmonized method for free T based on calculated free T using REVISED FORMULAE. This may bring the measurement of free T to a referable standard in clinical laboratories and common reference intervals that all clinicians can use
I don't have equilibrium dialysis assay in my country and they test free testosterone with RIA or CLIA method only So my recent free testosterone (RIA method) was 49 pg/ml ( 12-40 pg/ml) This says I am over the reference range . Should I take this for face value or assume the assay is...
www.excelmale.com
Take home points:
*Assays that are standardized are designed to provide accurate results, traceable to “true” value-assigned certified reference materials and gold-standard reference methods. Results obtained using standardized methods can be compared across assays, institutions, populations, and past and future test results, thereby improving diagnosis, treatment, and outcomes of patients
* Limitations of using free testosterone by equilibrium dialysis and calculated free testosterone concentrations in practice are the lack of assay standardization, an accuracy-based quality control program, and a harmonized reference range. Until these limitations are addressed, free testosterone by equilibrium dialysis and calculated free testosterone should use reference ranges established by individual laboratories or their specific assay method