madman
Super Moderator
Young men tend to have lower SHBG levels, and have less testosterone resistance on a cellular level, and therefore require less total testosterone to achieve healthy free T levels.
Regarding testosterone resistance again I stated my thoughts earlier. Leaving that aside.
You stated: "Young men tend to have lower SHBG levels, and have less testosterone resistance on a cellular level, and therefore require less total testosterone to achieve healthy free T levels.
True that having lower SHBG would require a lower TT to attain a healthy FT level and although having higher SHBG would result in one needing to hit a higher TT in order to achieve a healthy FT.....the TT level needed is not as high as most would think.
So let me get this right here.....as I stated to you many times before in men with highish/high SHBG an extremely high TT is in no way needed to achieve a healthy FT level due to the newer research/understanding of SHBG:T binding.
[0387] Relation between Percent FT with Total Testosterone and SHBG. Intra-dimer complex allostery suggests that SHBG can regulate FT fraction over a wide range of total testosterone concentrations without getting saturated. Indeed, it was found that percent FT calculated using the new model changed very modestly over a wide range of total testosterone concentrations. In contrast, the Vermeulen's equation suggests a negative relation between percent FT and total testosterone. Furthermore, as SHBG concentrations increase, percent FT calculated using our new model shows only a modest decline in contrast to the marked decline in percent FT calculated using Vermeulen's equation.
* Intra-dimer complex allostery suggests that SHBG can regulate FT fraction over a wide range of total testosterone concentrations without getting saturated.
*Furthermore, as SHBG concentrations increase, percent FT calculated using our new model shows only a modest decline
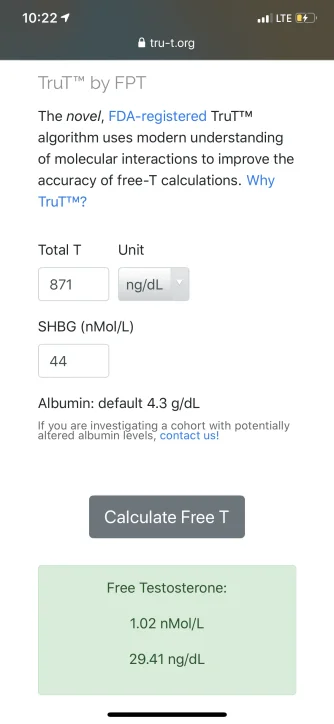
So lets take a man with high SHBG (70 nmol/L) and a pre-trt TT 600 ng/dL.
Using the newer calculated TruT method using a TT 600 ng/dL, SHBG 70 nmol/L, Albumin 4.3 g/dL (mean) than FT would be 16.56 ng/dL (borderline low in the reference range of 16-31 ng/dL).
.webp")
Now we take the same man and put him on trt using a dose of T injected twice weekly (every 3.5 days) that puts his TT 1000 ng/dL at TROUGH and for shits sake his SHBG does not budge 70 nmol/L, Albumin 4.3 g/dL (mean).
TT 1000 ng/dL, SHBG 70 nmol/L, Albumin 4.3 g/dL (mean) than FT would be 31.30 ng/dL (top end of the reference range 16-31 ng/dL).
So a man with a high SHBG of 70 nmol/L would only need a TT 1000 ng/dL to hit a healthy FT level at TROUGH in the (top end of the reference range).
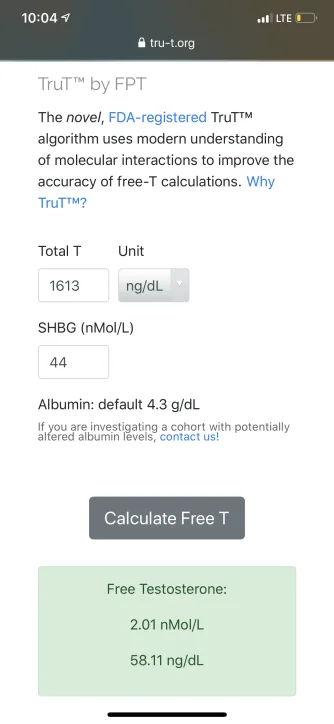
Using the same example if we bump his TT 1200 ng/dL and SHBG did not budge 70 nmol/L.
TT 1200 ng/dL, SHBG 70 nmol/L, Albumin 4.3 g/dL (mean) than his FT would be 38.86 ng/dL (over the top end of the reference range 16-31 ng/dL).
So again even if SHBG did not budge he would only need a TT 1200 ng/dL to hit a high FT level at TROUGH (over the top end of the reference range).
Most men suffering from low-t symptoms pre-trt depending on SHBG level either have low/low-normal TT with a low/sub-par FT or a descent TT with low/sub-par FT (due to high SHBG).
Using the newer calculated TruT method they would have low/low-normal FT levels whether in the 16-19 ng/dL range or much lower depend ones pre-trt (TT and SHBG) levels.
So you are going to tell me that if a man goes from a low or low/normal FT level pre-trt and that going on trt gets his FT of (9-12 ng/dL or say 16-19 ng/dL ) to 30--->30+ (high 30s).....keeping in mind that other hormones are healthy including thyroid/adrenal function.....that he is not going to experience relief/improvement in low-t symptoms let alone positive effects on ones overall health/well being?
Seems far fetched to me!
Highly doubtful most men would need a FT TROUGH 50-50+ ng/dL to experience the positive benefits of testosterone replacement therapy.
As you stated earlier:
"We just have to respect that we are all different. On the TOT roundtable fb group there are more guys than I can keep track of that still had symptoms when their free T was at the top of the range (even with the tru-T calculator) and didn’t have complete symptom resolution until their free T was almost double, if not double the top of the range. Then there are plenty of guys throughout the years that I’ve seen report they only achieved success when they lowered their dose. So again, we just have to respect that we are all very different, and may require different protocols to achieve symptom resolution"
Again highly doubtful one with low/low-normal FT would need to have their FT levels jacked up to double the top end of the reference range.....let alone at TROUGH to benefit from trt.
Seems almost ridiculous if one had FT <16 ng/dL or slightly higher all of a sudden needs levels of 50-50+ ng/dL to benefit in any way on trt!
Just to make myself clear I have no issue if one wants to run higher TT (1500+ ng/dL)/FT (50+ng/dL).....so be it to each his own but doubting it is truly needed.