shawncooke1
New Member
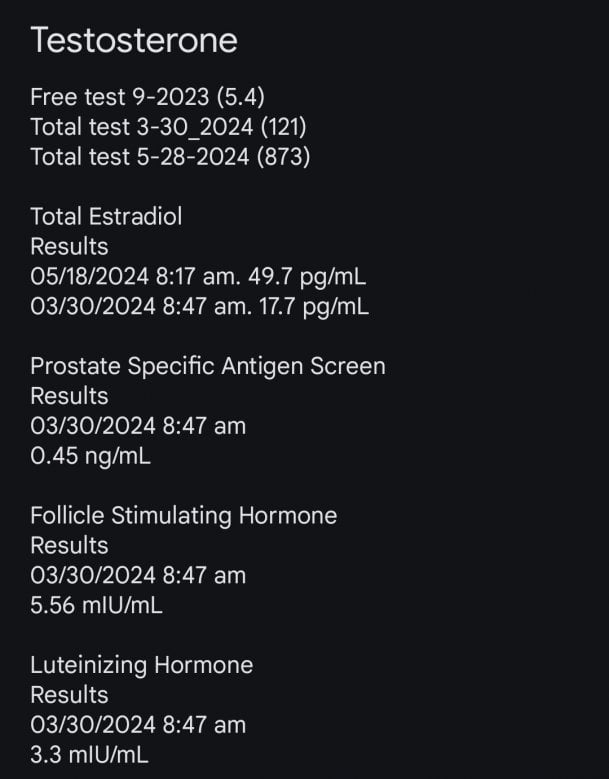
Hi, I'm new to the forum and new to try. In 2023 I was diagnosed with low testosterone and was prescribed a topical testosterone gell which didn't work. In fact my counts got lower after using it. So I went to a urologist and he ran some tests and decided I was a candidate for trt via cypionate. I was prescribed 100mg 1x per week intramuscular injections. My starting t was 121 and estradiol was 17.7. My 6 week blood work was 873T and 49.7 estradiol 5 days after my last shot. So I would assume that at some point I may have gotten to around 1000T before it started to fall off. I have a couple questions.
1. Should my Dr test my sbgh, because he hasn't.
2. Should he check my free testosterone, because he hasn't. My previous NP did prior to the gell and it was 5.4.
3. I'm at week 8 and haven't had much change in mood, libido or energy. Would 2x per week help me there? Could I be getting too much at once? He said that the estradiol was not concerning.
4. I've decided to do 50mg every 3.5 days to see if it helps. What will that do to my testosterone numbers? Will I still get up to around 1000 doing it that way or will it keep me lower but without the peaks and valleys?
5. I am not on any kind of blockers because he didn't see any harmful side effects yet. Is the estradiol a concern at those numbers?
Thanks in advance for any info that you can give.
1. Should my Dr test my sbgh, because he hasn't.
2. Should he check my free testosterone, because he hasn't. My previous NP did prior to the gell and it was 5.4.
3. I'm at week 8 and haven't had much change in mood, libido or energy. Would 2x per week help me there? Could I be getting too much at once? He said that the estradiol was not concerning.
4. I've decided to do 50mg every 3.5 days to see if it helps. What will that do to my testosterone numbers? Will I still get up to around 1000 doing it that way or will it keep me lower but without the peaks and valleys?
5. I am not on any kind of blockers because he didn't see any harmful side effects yet. Is the estradiol a concern at those numbers?
Thanks in advance for any info that you can give.