Hi everyone, I’m hoping some experienced members here can help me out.
I’ve been on TRT since August, prescribed by a UK clinic due to secondary hypogonadism. My testosterone levels were initially between 3 nmol and 9 nmol.
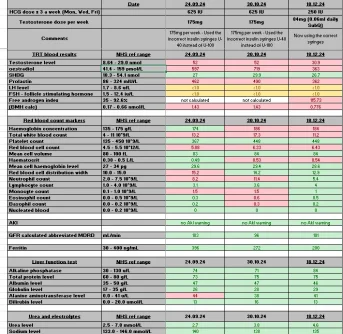
When I started treatment, I mistakenly took the wrong dose, which led to excessively high levels. It took about two months to realize this mistake. My testosterone shot up to over 52 nmol, and my E2 (estradiol) spiked to over 700 pmol/L. After realizing this, I lowered my dose to 84 mg of testosterone cypionate daily and 750 IU of HCG split into three doses weekly. After a month on this protocol, my RBC and testosterone levels were slightly above the upper range, but my E2 was still very high at 363 pmol/L.
The clinic then advised me to lower my testosterone to 56 mg per week (injected daily) and HCG to 500 IU per week, which I've split into daily injection.
I’ve been on this lower dose for two weeks now, but I feel absolutely awful. My body feels heavy, I’m constantly exhausted, and my libido has completely disappeared. I’ve spoken to the clinic about introducing an AI (aromatase inhibitor) because I suspect my E2 is still too high, but they want to avoid adding anything while I adjust to the lower doses.
Right now, I feel worse than I did before starting TRT. I have a 7-month-old baby and work responsibilities, but I’m struggling to get through the day—I feel like I need to sleep all the time. I’m starting to wonder if TRT just isn’t for me.
The main issues seem to be my high E2 and elevated RBC levels. I currently take daily aspirin, nattokinase (50 mg every other day), and 5 mg tadalafil daily to help mitigate clot risks. I also have a blood condition, hereditary spherocytosis, and no spleen, which puts me at a higher risk for blood clots.
Has anyone experienced something similar or have any advice? I’m limited in how often I can contact the clinic (understandably, to avoid overwhelming their inbox), so I’m trying to figure this out as best as I can.
I really wanted TRT to work for me, but I’m surprised I feel this bad. Is this just part of the process of finding the right balance on TRT?
- I’m 36 years old, 6’1” tall, and weigh around 19 stone.
- I weight train twice a week, focusing on heavy powerlifting-style lifts with some accessory work, and I also cycle once a week. However, I’m often too tired to train more frequently.
- I have hereditary spherocytosis and had my spleen removed, which increases my risk of blood clots.
- I don’t smoke or drink and generally lead a healthy lifestyle, though I do overindulge in food occasionally. I enjoy eating, and I’ve noticed that carbs seem to make me gain weight easily.
- I know I need to lose a few stone, and I’m actively working on it.
- I was on propranolol for two years, which contributed to weight gain. I started taking it after experiencing a few panic attacks around the time I realized I had low testosterone. At this time when i have 3nmol it felt like the wheels where falling on with my anxiety and health, it was sudden and come out of nowhere. (when i looked back at past blood test it was showing when i was 28 i was 12nmol total testosterone so not great then either.)
- Before starting TRT, I spent two years trying to improve my lifestyle in hopes of naturally raising my testosterone levels to a healthy range.
If anyone can share some knowledge or insight on what the F* is going on? some days i wake up and i just feel horrendous and very weak.
thank you
Luke
I’ve been on TRT since August, prescribed by a UK clinic due to secondary hypogonadism. My testosterone levels were initially between 3 nmol and 9 nmol.
When I started treatment, I mistakenly took the wrong dose, which led to excessively high levels. It took about two months to realize this mistake. My testosterone shot up to over 52 nmol, and my E2 (estradiol) spiked to over 700 pmol/L. After realizing this, I lowered my dose to 84 mg of testosterone cypionate daily and 750 IU of HCG split into three doses weekly. After a month on this protocol, my RBC and testosterone levels were slightly above the upper range, but my E2 was still very high at 363 pmol/L.
The clinic then advised me to lower my testosterone to 56 mg per week (injected daily) and HCG to 500 IU per week, which I've split into daily injection.
I’ve been on this lower dose for two weeks now, but I feel absolutely awful. My body feels heavy, I’m constantly exhausted, and my libido has completely disappeared. I’ve spoken to the clinic about introducing an AI (aromatase inhibitor) because I suspect my E2 is still too high, but they want to avoid adding anything while I adjust to the lower doses.
Right now, I feel worse than I did before starting TRT. I have a 7-month-old baby and work responsibilities, but I’m struggling to get through the day—I feel like I need to sleep all the time. I’m starting to wonder if TRT just isn’t for me.
The main issues seem to be my high E2 and elevated RBC levels. I currently take daily aspirin, nattokinase (50 mg every other day), and 5 mg tadalafil daily to help mitigate clot risks. I also have a blood condition, hereditary spherocytosis, and no spleen, which puts me at a higher risk for blood clots.
Has anyone experienced something similar or have any advice? I’m limited in how often I can contact the clinic (understandably, to avoid overwhelming their inbox), so I’m trying to figure this out as best as I can.
I really wanted TRT to work for me, but I’m surprised I feel this bad. Is this just part of the process of finding the right balance on TRT?
- I’m 36 years old, 6’1” tall, and weigh around 19 stone.
- I weight train twice a week, focusing on heavy powerlifting-style lifts with some accessory work, and I also cycle once a week. However, I’m often too tired to train more frequently.
- I have hereditary spherocytosis and had my spleen removed, which increases my risk of blood clots.
- I don’t smoke or drink and generally lead a healthy lifestyle, though I do overindulge in food occasionally. I enjoy eating, and I’ve noticed that carbs seem to make me gain weight easily.
- I know I need to lose a few stone, and I’m actively working on it.
- I was on propranolol for two years, which contributed to weight gain. I started taking it after experiencing a few panic attacks around the time I realized I had low testosterone. At this time when i have 3nmol it felt like the wheels where falling on with my anxiety and health, it was sudden and come out of nowhere. (when i looked back at past blood test it was showing when i was 28 i was 12nmol total testosterone so not great then either.)
- Before starting TRT, I spent two years trying to improve my lifestyle in hopes of naturally raising my testosterone levels to a healthy range.
If anyone can share some knowledge or insight on what the F* is going on? some days i wake up and i just feel horrendous and very weak.
thank you
Luke