Sorry to hear this.
When did you see him and what testing was done?
Did he performed your Doppler US examination?
Post your results from the Doppler.
If your peak systolic velocity (PSV) was borderline then your underlying vascular health would be at risk if you were not taking measures (lifestyle/underlying health issues) to address such.
You stated:
I have issues where I have erections that are about a 6 out of 10 on a scale.
Sometimes I have a day or two where I have a good strong erection but many days I don't.
My labs are attached.
I take 160/40 Testosterone cypionate propionate blend from empower. .08 ml daily.
I also take a daily tadalafil 20mg. Losartan 25 mg. Crestor 5 mg. Wellbutrin 300 mg. Dexilant 60mg.
You are taking tadalafil let alone a whopping daily dose which in most cases would most likely mean that you need a higher dose for it to be effective which indicates that you have some degree of vascular/endothelial dysfunction.
Your erections are 6/10 not too far off from a 5/10 and this is with a whopping dose of tadalafil so where would you truly sit without the use of a PDE5i?
Ones underlying vascular health/generation or bioavailability of NO will play a strong role in how well you respond to said dose.
You are also taking medications to control high blood pressure, high cholesterol, acid reflux and depression (MDD/SAD).
Even though lack of nocturnal erections/morning wood would indicate hormonal as it is common in men with low testosterone,
high levels of T let alone DHT are not needed for healthy erectile function/libido which was the point being stressed.
Again everyone so caught up on T, DHT and estradiol LMFAO! Much more involved than just having healthy hormones! One of the top in the field love this guy! Mulhall always breaks it down! Listen closely as he hits the nail on the HEAD! 3:33-7:13 * if you look at men with ORGANIC ED we can...

www.excelmale.com
3:33-7:13
* if you look at men with ORGANIC ED we can talk about psychogenic ED a little later on if we have time but if you take men with ORGANIC ED PROBABLY 70% OF THEM ARE GOING TO HAVE A VASCULAR COMPONENT INFLOW OR OUTFLOW PROBLEMS and that includes men with diabetes, those high profile causes like medication induced or hormonal ED or Arteriogenic ED, radical pelvic surgery for example account for the vast minority of patients with erectile dysfunction and if you focus in on HORMONE PROBLEMS such as TESTOSTERONE that accounts for the VAST MINORITY of MEN with ERECTION PROBLEMS so the BULK of ED that's PHYSICALLY BASED is VASCULOGENIC as its called!
* the whole link between TESTOSTERONE and ERECTILE FUNCTION it's a WEAK LINK, it's not a POTENT ERECTO-GENIC HORMONE, it's CERTAINLY a LIBDO-GENIC HORMONE and an ORGASMO-GENIC HORMONE but if you take men who have got LOW TESTOSTERONE who have ERECTILE DYSFUNCTION and you treat them with T the AVERAGE CHANGE in ERECTILE FUNCTION is MINIMAL if you use the validated scores (the international index of erectile function scores) so the ELEVATION in those scores is MINIMAL so the CONTRIBUTION of T you DON'T NEED A LOT of T you need SOME you DON'T NEED A LOT of T for ERECTION FUNCTION!
What role does DHT (dihydrotestosterone) play with erections?
9:33-11:54
* it is CERTAINLY ALL ANDROGENS are involved in ERECTILE TISSUE HEALTH and ERECTILE FUNCTION but as an ANDROGEN PERTAINING SPECIFICALLY to ERECTILE HEALTH it is NOT the MAJOR PLAYER TESTOSTERONE ITSELF would be MORE IMPORTANT!
It's a f**KING BIG MYTH still being pushed by all those sheep stinking up the so called men's health/HRT forums with that more T is better mentality!
You know the ones loaded with all those blast n cruizzzers those grown ass men abusing T/AAS!
Most of those so called HRT GURUs polluting the net let alone RUN of the MILL T-CLINICS are caught up on that sheep mentality!
Pure nonsense!
Need to tread lightly on who you take advice from when it comes to this HRT SHIT SHOW GAME!
Also keep in mind that it is not a given that everyone will experience morning wood 7 days a week as it is more common when you wake up during REM stage of sleep as this is when nocturnal erections peak.
What is more important is that you are having nocturnal erections throughout the night.
Neurotransmitters, vascular health, and healthy hormones all play a big role in erectile function/libido.
As you should know getting quality sleep is also critical.
Many men over 40 suffering from ED have some degree of vascular/endothelial dysfunction/reduced generation or bioavailability of NO.
Depending on the severity this can be overcome to some degree with the use of PDE5i/intracavernosal injections and in cases that are more severe worst case scenario would be a penile implant.
First line therapy for treating ED would be oral therapy and when it is no longer effective the next step would be intracavernosal injections or in some cases oral combined with ICI the final step for severe cases that do not respond to first or second line therapies would be surgery for placement of a penile implant!
As you would know high blood pressure, hyperlipidemia and high homocysteine are big markers for contributing to vascular/endothelial dysfunction, luckily you are treating such!
Bupropion can have a positive impact on libido due to its effects on neurotransmitters mainly dopamine but it is not a given in every case!
Even then looking over your protocol although I see no issue with one running a high-end/high trough FT within reason if they are not experiencing any sides let alone blood markers remain healthy but you are clearly struggling with issues (ED, elevated RBCs, hemoglobin and hematocrit) with borderline ferritin to boot!
You need to keep in mind although you are injecting daily your trough FT is high steady-state seeing as you are injecting a TC/TP blend.
Point here being is running a high-end/high trough FT steady-state can easily have a negative impact on erectile function let alone libido due to hammering the SHIT out of your DOPAMINE 24/7!
We are not talking about a short-lived daily peak here!
Again T also has a tonic effect on the CNS and can easily make one feel amped up which can stress the nervous system.
The body was never meant to be jacked up on T 24/7!
Again if you have no underlying issues (OSA, COPD, smoking) then your RBCs, hemoglobin and hematocrit are high due you high steady-state FT.
This has been an ongoing issue with you on here due to being caught up on that more T is better mentality.
Your estradiol is high due to your high FT which would be expected.
Your TIBC, iron saturation is high, normal iron and borderline low ferritin.
Are you still donating blood and if so when was your most recent donation.
Calcium, protein and albumin, A1C just over the top-end.
Need to address that very high homocysteine.
Low uric acid.
If you want to kill 2 birds with one stone as in struggling with the elevated hematocrit and hammering the shit out of your dopamine then I would strongly suggest giving oral TU (
Kyzatrex) a go!
Two daily short-lived peaks with long trough times while at the same time achieving a high-end TT/FT (depending on the dose) and increasing DHT to boot!
400 mg BID is most likely where its unless you are one of those hyper responders who will fare well on a lower daily dose!
All, I react very badly to injectable T (56 hematocrit @ 100 mg split 3x per week SubQ). My ferritin suffers greatly here and sits in the 20's to low 30's. I want it to be above 70. Testosterone have given me a severe case of periodic limb movement disorder due to low dopamine resulting (I...
www.excelmale.com
Hot off the press! You heard it here first, Nelson's domain is where it's at! High-dosed oral TU (
Kyzatrex 400 mg) BID, LH/FSH while lower were maintained at non-zero levels, minimal impact on hematocrit! *At a mean follow up time of 6 months, patients demonstrated a significant increase in...
www.excelmale.com


 Screenshot_20241127_165847_Edge.webp79.3 KB · Views: 72
Screenshot_20241127_165847_Edge.webp79.3 KB · Views: 72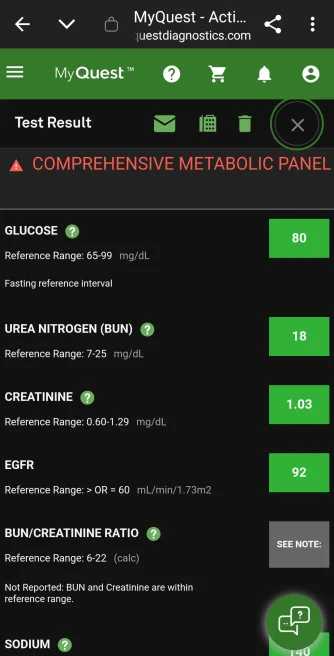 Screenshot_20241127_165902_Edge.webp81.7 KB · Views: 55
Screenshot_20241127_165902_Edge.webp81.7 KB · Views: 55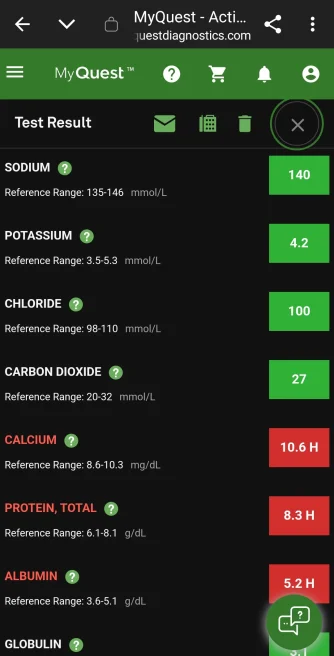 Screenshot_20241127_165915_Edge.webp78.7 KB · Views: 52
Screenshot_20241127_165915_Edge.webp78.7 KB · Views: 52 Screenshot_20241127_165920_Edge.webp80 KB · Views: 61
Screenshot_20241127_165920_Edge.webp80 KB · Views: 61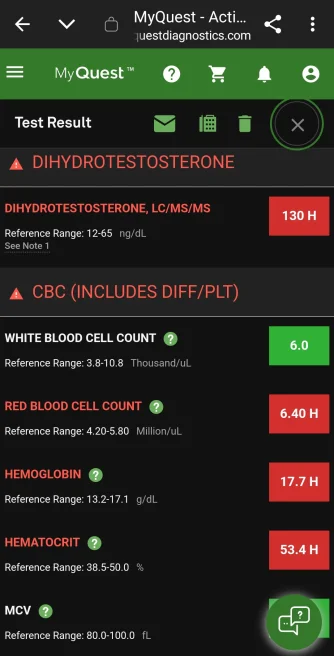 Screenshot_20241127_165928_Edge.webp90.1 KB · Views: 59
Screenshot_20241127_165928_Edge.webp90.1 KB · Views: 59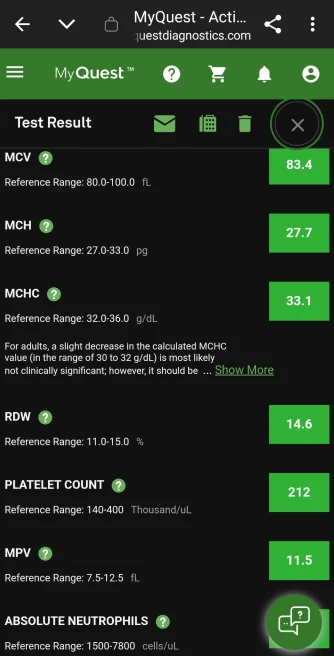 Screenshot_20241127_165941_Edge.webp87.3 KB · Views: 59
Screenshot_20241127_165941_Edge.webp87.3 KB · Views: 59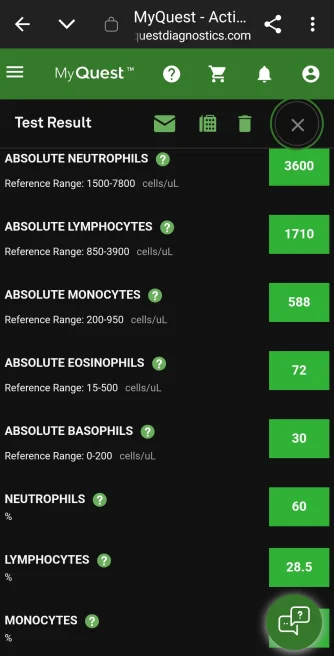 Screenshot_20241127_165947_Edge.webp79.6 KB · Views: 51
Screenshot_20241127_165947_Edge.webp79.6 KB · Views: 51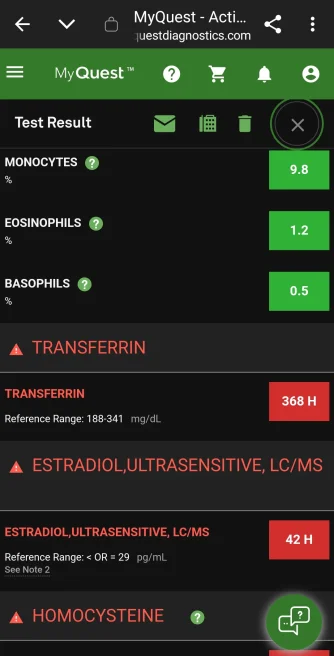 Screenshot_20241127_165954_Edge.webp75.2 KB · Views: 55
Screenshot_20241127_165954_Edge.webp75.2 KB · Views: 55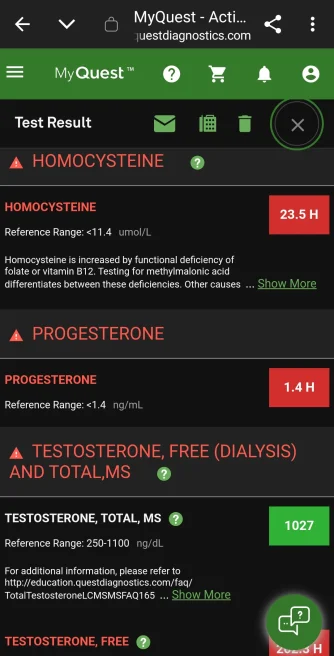 Screenshot_20241127_165959_Edge.webp112.1 KB · Views: 62
Screenshot_20241127_165959_Edge.webp112.1 KB · Views: 62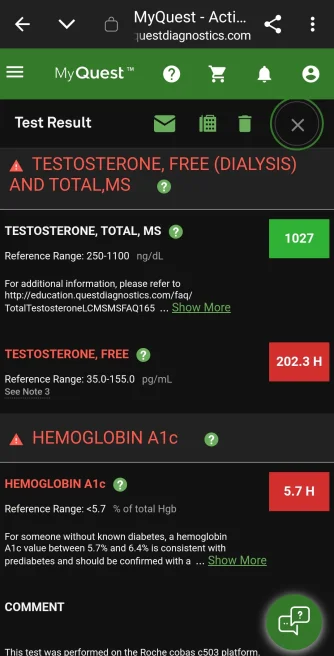 Screenshot_20241127_170004_Edge.webp112.6 KB · Views: 68
Screenshot_20241127_170004_Edge.webp112.6 KB · Views: 68











