I hate to chime in on this, given that I respect many of the posters and knowledge they provide, but there is a great deal of misinformation presented here.
This is misleading. If the thermostat clicks on when estrogen (E) is too low, then men with an androgen deficiency would, from concomitant low estradiol, experience an elevated LH pulse. The mistake here is that the "thermostat clicks on" in eugonadal men only. With secondary hypogonadism, where clomiphene citrate is normally indicated, the level of E deficiency required to "click on the thermostat" is substantially reduced and irregular. The thermostat is NOT operating properly. If it were working properly, there wouldn't be secondary hypogonadism in the first place.
Except, with secondary hypogonadism, T and E2 levels are already inadequate and yet the thermostat is already "off." Again, the thermostat is broken. We have to virtually starve it of E2 to get it to work properly.
The action of testosterone on the hypothalamus is mostly indirect, versus direct AR stimulation, and vastly, vastly less than the inhibitory effect of E2. In fact, T mostly affects the pulse frequency of LH and does not significantly attenuate the pulse amplitude. E2, however, affects amplitude. Regardless, per studies, it requires BOTH E2 and T to be sufficient to cause feedback. E2 insufficiency will still amplify the LH pulse even when T is normalized. In fact, that's why men on Clomid can have normal LH along with normal T and E.
This is false. Normal testosterone levels alone will not suppress the HPTA when E2 is blocked from inhibiting the LH pulse hypothalamus. Clomid will succeed in convincing the hypothalamus of an imbalance and LH will increase.
It will only increase marginally, however, because the LH will cause T/E2 to increase to the point of actual hypothalamic suppression. You'll hit a wall.
So, what actually interrupts the MoA of of Clomid? Extremely elevated androgens (steroids/supraphysiological FT) or significantly elevated free estradiol.
Normal T will NOT suppress LH without E2 also being normal, and in such a case — Clomid will always falsify E2 to the hypothalamus and cause it to panic.
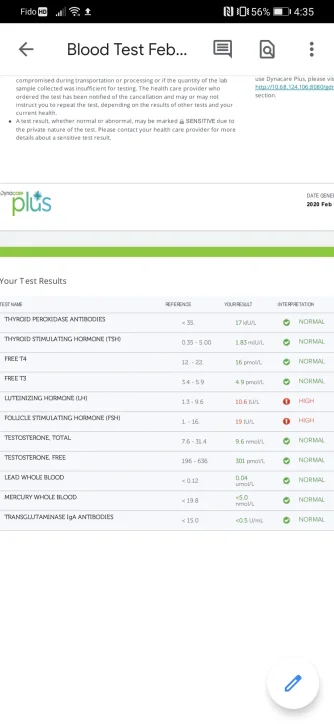
I have the labs to prove it, because I have used this combination myself. Apparently, so have other people in this thread. LH does return, but not fully.
I don't know why this myth persists. It requires a severely fundamental misunderstanding of the HPTA.