

Nelson Vergel
Founder, ExcelMale.com
Prolactin: Should Men with Erectile Dysfunction Be Tested ?
Prolactin is a hormone produced in the pituitary gland that is known for supporting lactation in women but also have many other functions on immune response, myelin coating on nerves, and also enhances LH receptors on testicular Leydig cells so that testosterone can be produced.
Prolactin levels peak during REM sleep, and in the early morning. Levels can rise after exercise, meals, sexual intercourse, minor surgical procedures, or following epileptic seizures.
High prolactin can decrease testosterone and cause sexual dysfunction.
Low Levels of Prolactin- Health Consequences
Prolactin (PRL) has been long deemed as a hormone involved only in female reproduction. However, PRL is a surprising hormone and, since its identification in the 1970s, its attributed functions have greatly increased. However, its specific role in male health is still widely unknown. Recently, low PRL has been associated with reduced ejaculate and seminal vesicle volume in infertile subjects. In addition, in men consulting for sexual dysfunction, hypoprolactinemia (low PRL) has been associated with erectile dysfunction and premature ejaculation, findings further confirmed in the general European population and infertile men. Several metabolic derangements, recapitulating metabolic syndrome, have also been associated with low PRL both in men with sexual dysfunction and from the general European population. In men with sexual dysfunction, followed-up for more than 4 years, low PRL was identified as an independent predictor of the incidence of major adverse cardiovascular events. Finally, an association with anxiety or depressive symptoms has been found in men with sexual dysfunction and from the general European population. While a direct role for impaired PRL function in the pathogenesis of these reproductive, sexual, metabolic and psychological disorders is conceivable, the possibility that low PRL is a mirror of an increased dopaminergic or a decreased serotonergic tone cannot be ruled-out. Hyperactivity of the dopaminergic system can explain only a few of the aforementioned findings, whereas a hypo-serotonergic tone fits well with the clinical features associated with low PRL, and there is significant evidence supporting the hypothesis that PRL could be a mirror of serotonin in the brain.
Normal prolactin blood level in men range between 2 and 18 ng/dL
High blood levels of prolactin are more common than low levels. Hyperprolactinemia (Prolactin > 150 ng/dL) is the most frequent abnormality of the anterior pituitary tumors, termed prolactinomas. Prolactinomas may disrupt the hypothalamic-pituitary-gonadal axis as prolactin tends to suppress the secretion of gonadotropin releasing hormone (GnRH– hormone responsible for activating the pituitary to male Luteinizing and Follicle Stimulating hormones- LH and FSH) therefore causing low testosterone and sperm production. Such hormonal changes may manifest as impotence in males. Inappropriate lactation in men is another important clinical sign of prolactinomas (yes, men’s breast tissue can produce small amounts of milk if high prolactin blood levels are present).
Substantial elevation in prolactin (>150 ng/mL) usually indicates a pituitary tumor. Very high levels of prolactin are associated with larger tumors. Prolactinomas are classified as microadenomas (<10 mm) and macroadenomas (>10 mm). The finding of a substantial elevation in blood levels of prolactin association with a pituitary lesion larger than 10 mm by radiographic analysis supports the diagnosis of a macroprolactinoma.
Modest levels of prolactin elevation (25–100 ng/mL) may be associated with several diagnoses. All other causes of hyperprolactinemia should be excluded before a tumor is considered. Primary hypothyroidism and chronic renal disease is associated with elevations in prolactin, probably because of altered metabolism or clearance of prolactin.
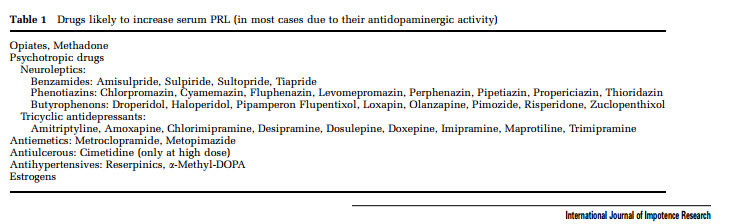
Some medications can increase prolactin blood levels in men, as shown in this table (source: Pharmacological causes of hyperprolactinemia)
Who Should Be Tested for High Prolactin:
1- Men not on testosterone replacement therapy (TRT) with very low levels of total testosterone (T level <150 ng/dL), especially if lower than normal LH is observed. For such male patients, testing for prolactin is used as screening for a potential pituitary gland problem (these men are referred to MRI)
2- Men with fluid production from their nipples. This has been observed in some men on anabolic steroids.
3- Men who have been on optimized TRT (TT levels above 500 ng/dL with free testosterone > 2 percent of TT) who complain of erectile dysfunction after at least 8-12 weeks of therapy. Prolactin is not usually included in baseline lab work due to cost and the fact that the incidence of high prolactin in men is about 5 percent, making it not economically justified. However, if baseline total testosterone is very low or optimized TRT fails to improve ED, prolactin testing could be justified.
Treatment of High Prolactin:
Due to its long half life and strong attachment to the prolactin receptor, the use of cabergoline at 0.25- 1 mg per week has become the main treatment of choice as a way to decrease prolactin in men on TRT.
Cabergoline (brand names Dostinex and Cabaser), an ergot derivative, is a potent dopamine receptor agonist on D2 receptors. In vitro, rat studies show cabergoline has a direct inhibitory effect on pituitary lactotroph (prolactin) cells. It is frequently used as a first-line agent in the management of prolactinomas due to higher affinity for D2 receptor sites, less severe side effects, and more convenient dosing schedule than the older treatment for this condition (bromocriptine).
In a small study done in men with very high prolactin (>1000 ng/dL) due to a pituitary tumor, a escalating dosing regimen of cabergoline improved prolactin and sexual function.
In another pilot study that enrolled men with ED who had with a median prolactin blood level of 31 ng/dL, a dose of 0.5 mg twice daily of cabergoline brought levels down to a median of 4.9 ng/dL and improved sexual function.
It is advisable to start at 0.2-0.5 mg once per week and then recheck blood levels after 4 weeks to ensure that prolactin is not reduced under 2 ng/dL (both high and low prolactin can cause ED).
Note: Some online forums have fueled the unmonitored use of cabergoline as a way to boost erectile function and decrease refractory (the time that takes to recover before having sex again) time after an orgasm. My concern with unmonitored use of this drug is that men may be driving their prolactin too low which results in the opposite effect they are seeking.
The post Prolactin: Should Men with Erectile Dysfunction Be Tested ? appeared first on Testosterone Wisdom.
Continue reading...
Prolactin is a hormone produced in the pituitary gland that is known for supporting lactation in women but also have many other functions on immune response, myelin coating on nerves, and also enhances LH receptors on testicular Leydig cells so that testosterone can be produced.
Prolactin levels peak during REM sleep, and in the early morning. Levels can rise after exercise, meals, sexual intercourse, minor surgical procedures, or following epileptic seizures.
High prolactin can decrease testosterone and cause sexual dysfunction.
Low Levels of Prolactin- Health Consequences
Prolactin (PRL) has been long deemed as a hormone involved only in female reproduction. However, PRL is a surprising hormone and, since its identification in the 1970s, its attributed functions have greatly increased. However, its specific role in male health is still widely unknown. Recently, low PRL has been associated with reduced ejaculate and seminal vesicle volume in infertile subjects. In addition, in men consulting for sexual dysfunction, hypoprolactinemia (low PRL) has been associated with erectile dysfunction and premature ejaculation, findings further confirmed in the general European population and infertile men. Several metabolic derangements, recapitulating metabolic syndrome, have also been associated with low PRL both in men with sexual dysfunction and from the general European population. In men with sexual dysfunction, followed-up for more than 4 years, low PRL was identified as an independent predictor of the incidence of major adverse cardiovascular events. Finally, an association with anxiety or depressive symptoms has been found in men with sexual dysfunction and from the general European population. While a direct role for impaired PRL function in the pathogenesis of these reproductive, sexual, metabolic and psychological disorders is conceivable, the possibility that low PRL is a mirror of an increased dopaminergic or a decreased serotonergic tone cannot be ruled-out. Hyperactivity of the dopaminergic system can explain only a few of the aforementioned findings, whereas a hypo-serotonergic tone fits well with the clinical features associated with low PRL, and there is significant evidence supporting the hypothesis that PRL could be a mirror of serotonin in the brain.
Normal prolactin blood level in men range between 2 and 18 ng/dL
High blood levels of prolactin are more common than low levels. Hyperprolactinemia (Prolactin > 150 ng/dL) is the most frequent abnormality of the anterior pituitary tumors, termed prolactinomas. Prolactinomas may disrupt the hypothalamic-pituitary-gonadal axis as prolactin tends to suppress the secretion of gonadotropin releasing hormone (GnRH– hormone responsible for activating the pituitary to male Luteinizing and Follicle Stimulating hormones- LH and FSH) therefore causing low testosterone and sperm production. Such hormonal changes may manifest as impotence in males. Inappropriate lactation in men is another important clinical sign of prolactinomas (yes, men’s breast tissue can produce small amounts of milk if high prolactin blood levels are present).
Substantial elevation in prolactin (>150 ng/mL) usually indicates a pituitary tumor. Very high levels of prolactin are associated with larger tumors. Prolactinomas are classified as microadenomas (<10 mm) and macroadenomas (>10 mm). The finding of a substantial elevation in blood levels of prolactin association with a pituitary lesion larger than 10 mm by radiographic analysis supports the diagnosis of a macroprolactinoma.
Modest levels of prolactin elevation (25–100 ng/mL) may be associated with several diagnoses. All other causes of hyperprolactinemia should be excluded before a tumor is considered. Primary hypothyroidism and chronic renal disease is associated with elevations in prolactin, probably because of altered metabolism or clearance of prolactin.
Some medications can increase prolactin blood levels in men, as shown in this table (source: Pharmacological causes of hyperprolactinemia)
Who Should Be Tested for High Prolactin:
1- Men not on testosterone replacement therapy (TRT) with very low levels of total testosterone (T level <150 ng/dL), especially if lower than normal LH is observed. For such male patients, testing for prolactin is used as screening for a potential pituitary gland problem (these men are referred to MRI)
2- Men with fluid production from their nipples. This has been observed in some men on anabolic steroids.
3- Men who have been on optimized TRT (TT levels above 500 ng/dL with free testosterone > 2 percent of TT) who complain of erectile dysfunction after at least 8-12 weeks of therapy. Prolactin is not usually included in baseline lab work due to cost and the fact that the incidence of high prolactin in men is about 5 percent, making it not economically justified. However, if baseline total testosterone is very low or optimized TRT fails to improve ED, prolactin testing could be justified.
Treatment of High Prolactin:
Due to its long half life and strong attachment to the prolactin receptor, the use of cabergoline at 0.25- 1 mg per week has become the main treatment of choice as a way to decrease prolactin in men on TRT.
Cabergoline (brand names Dostinex and Cabaser), an ergot derivative, is a potent dopamine receptor agonist on D2 receptors. In vitro, rat studies show cabergoline has a direct inhibitory effect on pituitary lactotroph (prolactin) cells. It is frequently used as a first-line agent in the management of prolactinomas due to higher affinity for D2 receptor sites, less severe side effects, and more convenient dosing schedule than the older treatment for this condition (bromocriptine).
In a small study done in men with very high prolactin (>1000 ng/dL) due to a pituitary tumor, a escalating dosing regimen of cabergoline improved prolactin and sexual function.
In another pilot study that enrolled men with ED who had with a median prolactin blood level of 31 ng/dL, a dose of 0.5 mg twice daily of cabergoline brought levels down to a median of 4.9 ng/dL and improved sexual function.
It is advisable to start at 0.2-0.5 mg once per week and then recheck blood levels after 4 weeks to ensure that prolactin is not reduced under 2 ng/dL (both high and low prolactin can cause ED).
Note: Some online forums have fueled the unmonitored use of cabergoline as a way to boost erectile function and decrease refractory (the time that takes to recover before having sex again) time after an orgasm. My concern with unmonitored use of this drug is that men may be driving their prolactin too low which results in the opposite effect they are seeking.
The post Prolactin: Should Men with Erectile Dysfunction Be Tested ? appeared first on Testosterone Wisdom.
Continue reading...














