I am on TRT 100mg/week .25 alanstrozole. I also take Ambien, Antihistamin, melatonin.
Does ambien cause hair loss if anyone aware of ? I am losing hair since I got on TRT, slow getiing male pattern baldness. My father was not bald. So its not related to gene.
Anastrozole causes hair loss, in fact a large percentage of women report hair loss on anastrozole during the course of treatment.
TRT can accelerate hair loss. My brother lost his hair at a young age and no one else in the family lost their hair even later in life, so just because your father didn't lose his hair in no way spares you from losing yours.
TRT increases DHT the culprit in male hair loss (on the head) and Anastrozole as Systemlord stated. And definitely hair inheritance is complex. My boys should have been bald from my ancestors genetics. Miraculously, they dodged that genetic bullet.
Anastrozole causes hair loss, in fact a large percentage of women report hair loss on anastrozole during the course of treatment.
TRT can accelerate hair loss. My brother lost his hair at a young age and no one else in the family lost their hair even later in life, so just because your father didn't lose his hair in no way spares you from losing yours.
Yes my mom's side has baldness issue. Most of my maternal uncles are kinda bald. I did not know that anastrozole can also cause hair loss issue in men. I thought only DHT is the culprit.
I am on TRT 100mg/week .25 alanstrozole. I also take Ambien, Antihistamin, melatonin.
Does ambien cause hair loss if anyone aware of ? I am losing hair since I got on TRT, slow getiing male pattern baldness. My father was not bald. So its not related to gene.
Yes my mom's side has baldness issue. Most of my maternal uncles are kinda bald. I did not know that anastrozole can also cause hair loss issue in men. I thought only DHT is the culprit.
I would appreciate any professional opinion on adding nandrolone to TRT to help attenuate high DHT symptoms, specifically acne. For example; If the current protocol was 100mg of a testosterone ester per week. With the protocol being ideal, but for the acne due to DHT conversion. Would...
*Sometime later in life, and with the contribution of a genetic predisposition, androgen activity in the scalp may also help to initiate male-pattern hair loss.It is a misconception that dihydrotestosterone is an isolated culprit in the promotion of hair loss, however; as in actuality, it is the general activation of the androgen receptor that is to blame (see DHT Conversion).
*Acne, for example, is often triggered by dihydrotestosterone activity in the sebaceous glands, and the local formation of dihydrotestosterone in the scalp is typically blamed for triggering male pattern hair loss. You should know that it is a terrible misconception among bodybuilders that dihydrotestosterone is an isolated culprit when it comes to these side effects.All anabolic/androgenic steroids exert their activities, both anabolic and androgenic, through the same cellular androgen receptor"
*Dihydrotestosterone is no different than any other steroid except that it is a more potent activator of this receptor than most, and can be formed locally in certain androgen-sensitive tissues.All steroids can cause androgenic side effects in direct relation to their affinity for this receptor, and DHT has no known unique ability in this regard"
I saw a video on youtube one doctor saying that one can regrow dead follicle and regrow new hair with the help of supplementing Biotin, Vitamin E, Zinc, Ginseng, Niacin. I am skeptical about it.
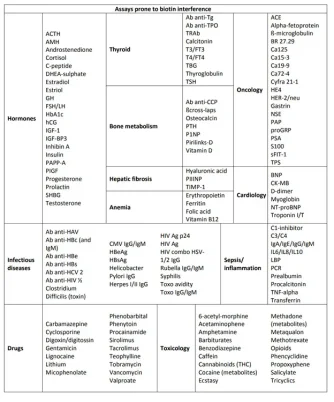
But keep in mind that Biotin causes interfere with some blood works.
Personally, I've never subscribed to the DHT 'genetic susceptibility' theory of male pattern baldness. Androgens are undoubtably involved on some level, but there's too much data associating increased prolactin, cortisol, aldosterone and estrogen (systemic, not scalp), calcification of the vasculature, localized hypoxia in balding vs non-balding skin, scalp fibrosis, etc, etc, for it to be that simple.
As well as being an androgen antagonist, progesterone possess anti-calcification, -fibrosis, -estrogen, -gluco and -mineralocorticoid activity, whilst also opposing hypoxia by facilitating efficient oxidative respiration (i.e, increased CO2 production, which by-proxy oxygenizes tissue via the bohr effect). Given women start to lose their hair in an androgenic pattern post-menopause - a period of progesterone deficiency with marked increase in tissue stores of estrogen despite decreased ovarian output - I believe it's central to the pathophysiology, and the reason they're protected from MPB in youth.
Just my thoughts; not claiming anything as factual and/or absolute. I'll be experimenting with topical progesterone soon, but I don't envision it doing much since MPB seems more so a systemic issue. Will keep the forum updated.
Personally, I've never subscribed to the DHT 'genetic susceptibility' theory of male pattern baldness. Androgens are undoubtably involved on some level, but there's too much data associating increased prolactin, cortisol, aldosterone and estrogen (systemic, not scalp), calcification of the vasculature, localized hypoxia in balding vs non-balding skin, scalp fibrosis, etc, etc, for it to be that simple.
As well as being an androgen antagonist, progesterone possess anti-calcification, -fibrosis, -estrogen, -gluco and -mineralocorticoid activity, whilst also opposing hypoxia by facilitating efficient oxidative respiration (i.e, increased CO2 production, which by-proxy oxygenizes tissue via the bohr effect). Given women start to lose their hair in an androgenic pattern post-menopause - a period of progesterone deficiency with marked increase in tissue stores of estrogen despite decreased ovarian output - I believe it's central to the pathophysiology, and the reason they're protected from MPB in youth.
Just my thoughts; not claiming anything as factual and/or absolute. I'll be experimenting with topical progesterone soon, but I don't envision it doing much since MPB seems more so a systemic issue. Will keep the forum updated.
Why are u planning on experimenting with progesterone topically opposed to topically? Are u referring to applying it topically to ur scalp, or just skin in general?
Why are u planning on experimenting with progesterone topically opposed to topically? Are u referring to applying it topically to ur scalp, or just skin in general?
The application would be topically on the scalp itself, mainly in attempt to produce somewhat supraphysiologcal concentrations locally whilst keeping the rise in systemic levels physiological. I wouldn't be that concerned if serum levels were elevated though given it's a largely protective hormone - there'd just be the anti-libido / erectile effects to worry about through AR antagonism, but that's only temporary and dissipates as soon as the dose is lowered.
The application would be topically on the scalp itself, mainly in attempt to produce somewhat supraphysiologcal concentrations locally whilst keeping the rise in systemic levels physiological. I wouldn't be that concerned if serum levels were elevated though given it's a largely protective hormone - there'd just be the anti-libido / erectile effects to worry about through AR antagonism, but that's only temporary and dissipates as soon as the dose is lowered.
Ya progesterone is a tricky one. Some guys say it only gives them negative side effects, and others swear by it. Seems very similar to HCG. Some swear by HCG and say they don’t have a libido without it, and just don’t feel as good without it, and others hate the stuff and all it does is cause them side effects
U getting the topical progesterone over the counter or prescribed?
I just can't help but wonder if there's anything to the new scientific explanation and approach for treating hair loss (for men and women) by stimulating hair follicle stem cells with a cocktain of natural supplements by Dr Al Sears:
Not an endorsement, because I haven't tried this. So many products out there because guys will try anything to help this aging issue. Just curious about this one because of an alternate scientific expansion for the underlying cause.
Yes my mom's side has baldness issue. Most of my maternal uncles are kinda bald. I did not know that anastrozole can also cause hair loss issue in men. I thought only DHT is the culprit.
ABSTRACT Introduction: Androgenetic alopecia is a common hair loss disorder affecting up to 80% of males by the age of 80. It is characterized by androgen-related progressive thinning of hair in a defined pattern. It results in diminished self-esteem, reduced confidence, and distress in...
www.excelmale.com
6. Expert opinion
AGA occurs universally in all adult men and severity progresses with age. Twin studies have confirmed that the age of onset, severity, rate of progression, and pattern of hair loss are all influenced by inherited factors. Heredity is thought to contribute more than 80% to the AGA phenotype, while environmental factors account for less than 20%.AGA is inherited as a complex polygenic trait. Genome-wide association studies have identified over 190 genes that are thought to be involved in AGA,however, the first gene associated with AGA, the androgen receptor gene, is thought to account for over 60% of the heredity of AGA.
Personally, I've never subscribed to the DHT 'genetic susceptibility' theory of male pattern baldness. Androgens are undoubtably involved on some level, but there's too much data associating increased prolactin, cortisol, aldosterone and estrogen (systemic, not scalp), calcification of the vasculature, localized hypoxia in balding vs non-balding skin, scalp fibrosis, etc, etc, for it to be that simple.
As well as being an androgen antagonist, progesterone possess anti-calcification, -fibrosis, -estrogen, -gluco and -mineralocorticoid activity, whilst also opposing hypoxia by facilitating efficient oxidative respiration (i.e, increased CO2 production, which by-proxy oxygenizes tissue via the bohr effect). Given women start to lose their hair in an androgenic pattern post-menopause - a period of progesterone deficiency with marked increase in tissue stores of estrogen despite decreased ovarian output - I believe it's central to the pathophysiology, and the reason they're protected from MPB in youth.
Just my thoughts; not claiming anything as factual and/or absolute. I'll be experimenting with topical progesterone soon, but I don't envision it doing much sin
The application would be topically on the scalp itself, mainly in attempt to produce somewhat supraphysiologcal concentrations locally whilst keeping the rise in systemic levels physiological. I wouldn't be that concerned if serum levels were elevated though given it's a largely protective hormone - there'd just be the anti-libido / erectile effects to worry about through AR antagonism, but that's only temporary and dissipates as soon as the dose is lowered.
You maybe onto something here. I have wondered why DHT only seems to affect the scalp, and even there, not the sides, just the top. Whereas DHT seems to promote hair growth elsewhere on a man's body. Doesn't make sense. Why would it only stop hair growth on the top, crown and front of the head, and not the sides?
You maybe onto something here. I have wondered why DHT only seems to affect the scalp, and even there, not the sides, just the top. Whereas DHT seems to promote hair growth elsewhere on a man's body. Doesn't make sense. Why would it only stop hair growth on the top, crown and front of the head, and not the sides?
The genetic AGA model also fails to explain why the vast majority of men lose their hair as they age, when androgens fall and estrogen, prolactin, cortisol, etc, are all shown to rise - if genetic susceptibility + androgen receptor activation alone was the cause, men would bald in youth when androgens are at their highest, but they don't. The same paradox exists for androgens and prostate cancer, too.
I'm not trying to pretend that I know what causes MPB, nor how to treat it; but there's certainly more going on under the surface.
I possess a script for prog cream, but I'll likely go with the former since it's cheaper + less additives.
I've seen the same discrepancy between the effects of prog too - some dudes say it sends their libido through the roof, quells anxiety and facilitates great sleep, whereas others report the exact opposite.
Hard to know why, but my guess would be that most people take way too much. Ime, as little as 0.5mg per day is enough to put my prog levels above range two hours post application, so people who get bad sides from a 'low' dose of 5mg are probably sending their levels through the roof, or never needed it in the first place.
You maybe onto something here. I have wondered why DHT only seems to affect the scalp, and even there, not the sides, just the top. Whereas DHT seems to promote hair growth elsewhere on a man's body. Doesn't make sense. Why would it only stop hair growth on the top, crown and front of the head, and not the sides?
6.1 Introduction 6.2 Structure and function of the hair follicle 6.3 The paradoxical effects of androgens on human hair growth 6.4 The mechanism of androgen action in the hair follicle 6.5 The treatment of androgen-potentiated hair disorders 6.6 Key messages 6.7 References
ABSTRACT: Hair’s importance in human communication means that abnormalities like excess hair in hirsutism or hair loss in alopecia cause psychological distress. Androgens are the main regulator of human hair follicles, changing small vellus follicles producing tiny, virtually invisible hairs into larger intermediate and terminal follicles making bigger, pigmented hairs. The response to androgens varies with the body site as it is specific to the hair follicle itself. Normally around puberty, androgens stimulate axillary and pubic hair in both sexes, plus the beard, etc. in men, while later they may also inhibit scalp hair growth causing androgenetic alopecia. Androgens act within the follicle to alter the mesenchyme–epithelial cell interactions, changing the length of time the hair is growing, the dermal papilla size and dermal papilla cell, keratinocyte, and melanocyte activity. A greater understanding of the mechanisms of androgen action in follicles should improve therapies for poorly controlled hair disorders like hirsutism and alopecia.
Androgens have paradoxically different effects on human hair follicles
The importance of androgens is shown when pubertal pubic and axillary hair develops (8–10) in girls before boys (73,74), paralleling increasing circulating androgens. Testosterone also stimulates beard growth in eunuchs and elderly men (75), while castration inhibits beard (19) and balding (76). The roles of androgens and androgen receptors in adult hair is emphasized in XY individuals with complete androgen insufficiency, i.e., unable to respond to androgens due to dysfunctional androgen receptors (77); they develop a female-type phenotype, but lack pubic and axillary hair or androgenetic alopecia (FIG. 1). Sexual hair development is inhibited in growth hormone deficiency (78), suggesting that growth hormone is also essential.
When androgens stimulate the tiny vellus follicles to produce longer, thicker, more pigmented hairs (FIG. 2), the follicles must pass through the hair cycle, regenerating the lower follicle to carry out such changes (see “The hair follicle growth cycle”). Although androgens stimulate hair growth in many areas, causing greater hair on the face, upper pubic diamond, chest, etc. in men (19), they can also have the opposite effect on specific scalp areas, often in the same individual, causing balding (20). This involves a reverse transformation via hair follicle cycles, changing large, terminal follicles producing long, often heavily pigmented scalp hairs to miniaturized vellus follicles forming tiny, almost invisible hairs (FIG. 2). This balding usually occurs in men in a precise pattern starting with regression on the forehead and thinning in the center of the vertex and may continue exposing large areas of the scalp (20,79); the lower sides and back normally retain terminal hair. A different pattern of androgen-dependent alopecia may present in women; the frontal hairline usually remains unaffected while generalized thinning occurs on the central scalp and vertex (80) (FIG. 1). Androgenetic alopecia is reviewed elsewhere (14). At the same time, androgens have no apparent effect in other areas such as the eyelashes (FIG. 2). How does this paradoxical effect occur of one hormone frequently stimulating hair follicles, but also having no effect or inhibiting the same organ in the same person?
There are also significant differences between androgen-stimulated follicles. Female androgen levels affect axillary and lower pubic follicles, while other follicles require male levels (72,73). Follicle sensitivity also varies; facial follicles enlarge first above the mouth (mustache) and on the chin in boys and hirsute women, spreading gradually over the face and neck (10). Similar gradual progression occurs elsewhere taking many years to show the full response like on a man’s chest (19) or balding (20,79); terminal hairs may only appear on the ear canal in the fifties (49). Interestingly, these slow changes resemble the late androgen-dependent responses in the prostate-causing prostatic benign hypertrophy and carcinoma (81). Beard and axillary hair growth show another paradox; after their pubertal growth spurt, beard growth remains high, while axillary hair growth decreases rapidly in both sexes (19).
Why do follicles respond so differently?
These contrasts must be due to intrinsic differences in gene expression within follicles at different sites, since all receive the same circulating hormones and use the same receptors. A follicle’s retention of it's original androgen response when transplanted, the basis of cosmetic hair transplants, confirms this (82). Presumably, this genetic programming occurs during embryonic patterning processes. The molecular mechanisms involved in the development of different follicle types are not clear, but secreted signaling factors (such as Eda, sonic hedgehog, Wnt) and various growth factor families (like the BMPs), nuclear factors (including various homeobox genes), and others such as Hairless and Tabby, plus transmembrane and extracellular matrix molecules are all implicated (83,84).
Human follicles require androgens to initiate these marked changes.However, if adult men are castrated, although beard growth falls (19) and balding halts (85), neither returns to prepubertal levels, indicating that androgens have altered some gene expression permanently or that the lower androgen levels provided by the adrenals can maintain a partial effect. Increased summer beard growth (3), probably due to raised androgens (Seasonal changes in human hair growth), and inhibition of hirsutism (86) or regrowth stimulation in androgenetic alopecia (87,88) by drugs interfering with androgen action confirms that androgens are also needed to maintain follicular responses.
Genetics also appears important (reviewed in 1). Heavy beard growth (19) and balding (75) run in families and Caucasians generally exhibit more hair than Japanese (19) and more baldness than Africans (89). Several genes have been investigated for association with androgen-sensitive hair disorders with some links with those involved with androgen metabolism or receptors (reviewed (1)). Interestingly, women with polycystic ovaries and their brothers with early balding show a link to the steroid metabolism gene, CYP17 (90). A recent study of androgenetic alopecia families suggests a new susceptibility gene on chromosome locus 3q26 (91).
FIG. 1. Human hair patterns under differing endocrine conditions. Visible (i.e. terminal) hair with protective functions normally develops in children on the scalp, eyelashes, and eyebrows. Once puberty occurs, more terminal hair develops on the axilla and pubis in both sexes and on the face, chest, limbs, and often on the back in men. Androgens also stimulate hair loss from the scalp in men with the appropriate genes in a patterned manner causing androgenetic alopecia. People with various androgen insufficiency syndromes (lower panel) demonstrate that none of these occurs without functional androgen receptors and that only axillary and female patterns of lower pubic triangle hairs are formed in the absence of 5α-reductase type 2. Male pattern hair growth (hirsutism) occurs in women with abnormalities of plasma androgens or from idiopathic causes and women may also develop a different form of hair loss, female androgenetic alopecia. Reproduced from Randall 2000 (132).
FIG. 2. Androgens have paradoxically different effects on human hair follicles depending on their body site. During, and after, puberty androgens stimulate the gradual transformation of small follicles producing tiny, virtually colorless, vellus hairs to terminal follicles producing longer, thicker, and more pigmented hairs (upper panel) (19). These changes involve passing through the hair cycle (see FIG. 3). At the same time, many follicles on the scalp and eyelashes continue to produce the same type of hair, apparently unaffected by androgens (middle panel). In complete contrast, androgens may inhibit follicles on specific areas of the scalp in genetically susceptible individuals causing the reverse transformation of terminal follicles to vellus ones and androgenetic alopecia (20). Diagram reproduced from Randall 2000 (132).
FIG. 3. The hair follicle growth cycle. Hair follicles go through well-established repeated cycles of development and growth (anagen), regression (catagen), and rest (telogen) (1,2) to enable the replacement of hairs, often by another of differing color or size. An additional phase, exogen, has been reported where the resting club hair is released (42–44).
I possess a script for prog cream, but I'll likely go with the former since it's cheaper + less additives.
I've seen the same discrepancy between the effects of prog too - some dudes say it sends their libido through the roof, quells anxiety and facilitates great sleep, whereas others report the exact opposite.
Hard to know why, but my guess would be that most people take way too much. Ime, as little as 0.5mg per day is enough to put my prog levels above range two hours post application, so people who get bad sides from a 'low' dose of 5mg are probably sending their levels through the roof, or never needed it in the first place.

.png")







