

madman
Super Moderator
Efficient use of penile Doppler ultrasound for investigating men with erectile dysfunction
AbstractBackground. Vasculogenic erectile dysfunction is the most common type of erectile dysfunction, and penile Doppler ultrasound (PDUS) is a useful too
 academic.oup.com
academic.oup.com
Introduction
Current evidence demonstrates that >80% of patients with erectile dysfunction (ED) have some underlying organic etiology.1 Among organic causes, vasculogenic ED is the most common.1 Vasculogenic ED includes insufficient arterial inflow (arterial insufficiency), corporal veno-occlusive dysfunction (CVOD), or mixed vasculogenic ED (arterial insufficiency + CVOD).2 The guidelines of the American Urological Association and European Association of Urology for the evaluation of ED emphasize a comprehensive approach, beginning with a thorough medical, sexual, and psychosocial history, followed by a physical examination and selective laboratory testing. Expert opinion statements state that specialized testing may be required for individuals with more complex histories and presentations of ED. Among others, such advanced tests include penile Doppler ultrasound (PDUS).3-7 The European Association of Urology guidelines for sexual and reproductive health describe PDUS as a second level diagnostic test to evaluate the hemodynamics of erectile function, and it is usually used in conditions associated with a vasculogenic etiology of ED.7
PDUS assesses corpus cavernosal structure and function (hemodynamics)3 and has emerged as the gold standard for penile vascular assessment.4 In 1985 Lue et al first described PDUS using a pharmacologically induced erection as an alternative to the functional and anatomic studies available at the time—namely, dynamic infusion cavernosometry/cavernosography and selective internal pudendal arteriography.8
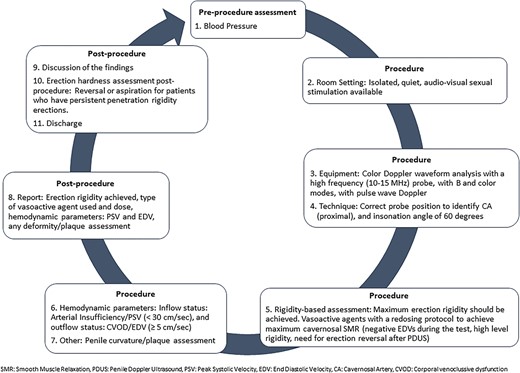
Despite decades since its introduction and efforts at standardizing the procedure, there remains great heterogeneity in PDUS protocols published in the literature: variability in the choice of intracavernosal vasoactive agent used, use of vasoactive agent redosing protocols, means of erectile rigidity assessment, timing of hemodynamic assessment, and hemodynamic parameter cutoffs.8-10 These discrepancies are a source of significant concern given the high rates of false diagnoses of abnormalities in erectile hemodynamics, particularly CVOD. For instance, in a study performed in patients with a CVOD diagnosis based on PDUS performed elsewhere, Teloken et al demonstrated a false diagnosis rate of 47%.11 This emphasizes the importance of having a standardized methodology for PDUS, which may aid in avoiding further unnecessary and potentially harmful interventions. Ensuring accurate hemodynamic diagnosis avoids patient exposure to improperly indicated selective internal pudendal arteriography or cardiologic investigation for an erroneous diagnosis of arterial insufficiency or the potential for unnecessary penile implant surgery in cases of a false diagnosis of CVOD. Figure 1 summarizes the critical points in using PDUS efficiently to evaluate erectile structure and function.
Indications
The purpose of PDUS is to define arterial inflow and/or venous outflow (veno-occlusive function) in men for whom knowing these diagnoses may change the patient prognosis discussion and/or therapeutic plan. PDUS proves invaluable in distinguishing non vasculogenic (normal hemodynamics,most often psychogenic ED) and vasculogenic etiologies.The accuracy of PDUS is predicated on the achievement of complete cavernosal smooth muscle relaxation (SMR), most often signified by high-end erection rigidity or the presence of negative end diastolic velocities (EDVs; Figure 2).12,13
*Procedural considerations
*Data interpretation
*Postprocedural considerations
Controversies
Gold standard for penile vascular assessment
PDUS represents the gold standard test for erectile hemodynamics assessment despite not being 100% accurate. Cavernosometry/cavernosography, a more sophisticated assessment of hemodynamics, is more invasive and equipment intensive, and in contemporary practice, few clinicians have experience in performing it and interpreting the data; thus, it has fallen out of favor.
*Normal hemodynamic parameter cutoffs
*Absence of age-based reference ranges
*Probe location
*Angle of insonation
*PDUS variability
*Training, performance, and interpretation
Take-home message
PDUS is a valuable minimally invasive tool for erectile hemodynamic assessment in men with ED and can aid in delineating the etiology of ED and thus guide its management. PDUS should be conducted only by clinicians who have received formal training in the performance of PDUS and analysis of the data generated. There is a dire need for standardization of PDUS protocols. Redosing of a vasoactive agent and the availability of audiovisual sexual stimulation are useful to maximize complete cavernosal SMR, which is critical for the generation of reliable data. For this reason, we suggest the utilization of a rigidity-based assessment during PDUS. PDUS should be performed after the patient achieves full erection hardness or the maximum dose of the vasoactive agent has been administered. We recommend a PSV cutoff of <30 cm/s to diagnose arterial insufficiency and an EDV cutoff of ≥5 cm/s to diagnose CVOD. Finally, all patients must achieve detumescence below penetration hardness before discharge.

.webp")










