

madman
Super Moderator
I have been on this site for several years and really appreciate all the info and opinions. Posted once several years ago about how “Gene’s Stack” helped me with some sexual function issues. I think increasing NO has helped my overall health in the years since. But the sexual issues have lingered and I've strongly considered TRT for years. I am pretty healthy and overall feel pretty good. Mood and energy is good, eat pretty healthy and workout 4-5 days per week. Play basketball twice a week and mix in weight training and yoga other days. My most recent numbers are…
57 years old
190 lbs
453 ng/dL total t
65.5 pg/dL free t
30 nmol/L shbg
132.2 ng/dL bio available t
My current doctor will not consider TRT at those numbers. But I recently met and talked to some guys locally who highly recommend I get on it. They suggested pellets or injections. From my research I would like to start with cream and see how it goes from there.
I have read many suggestions to newbies and people on the fence like me but curious to get opinions and suggestions from some of you about my specific numbers and situation.
Thank you in advance for your feedback.
Need to post reference ranges/assay used especially for free testosterone.
You need to test your FT using what would be considered the most accurate assay the gold standard Equilibrium Dialysis especially in cases of altered SHBG in order to know where your FT level truly sits.
This is critical!
Even then without knowing what assay was used as sammmy stated you can easily calculate it using your TT, SHBG and Albumin.
This can be done online for free using the linear law-of-mass action cFTV.
If we take your not so stellar TT 453 ng/dL, normal SHBG 30 nmol/L and Albumin 4.3 g/dL (default) then your cFTV would be 9.94 ng/dL which is not low but it is under where a healthy young male would sit which would be 13-15 ng/dL.
Even then no one cared to mention that cFTV tends to overestimate FT.
As I have stated numerous times on the forum you always have the option of using/relying upon calculated FT which would be the linear law-of-mass action cFTV as it has already been validated twice (1st time was done using TT/SHBG assays no longer available) and was then eventually re-validated using current state-of-the-art ED method (higher order reference method) let alone more recently against CDCs standardized Equilibrium Dialysis assay.
Yes it tends to overestimate slightly but it is nothing to fret over!
*Calculated free T using high-quality T and SHBG assays has been considered the most useful for clinical purposes [99]. All algorithms suffer from some inaccuracies, including the variable quality of SHBG IAs [100], not replicating the non-linear nature of T-SHBG binding, different and inaccurate association constants for SHBG and albumin binding [101], and variable agreement with equilibrium dialysis results [99,100]. However, until further developments in the field materialize, the linear model algorithms [in particular, the most used Vermeulen equation [102]] appear to give, despite a small systematic positive bias, acceptable data for the clinical management and research[37,103].
What is critical here is that you are hitting a cFT 9.94 ng/dL so if you had it tested using the most accurate assay (Equilibrium Dialysis) it would most likely be even lower as in 6-7 ng/dL which is low/bottom-end as most healthy young males would be hitting a FT 12 ng/dL.
Again just to put this in perspective most healthy young males would be hitting a FT 12 ng/dL tested using the gold standard Equilibrium Dialysis assay (most accurate) or a cFTV 13-15 ng/dL and this is a short-lived peak to boot!
Trough would be 20-25% lower.
More importantly a FT in the low-mid 20s whether cFTV or standardized ED assay would be high!
Again everyone needs to hammer it in their heads that a TROUGH FT 30 ng/dL is absurdly high.
We are talking TROUGH here too not peak!
Everyone so caught up on thinking they need to be hitting these high/absurdly high troughs to have this so called stellar libido!
Libido let alone erectile function are much more complex!
Again having a healthy FT is only one piece of the puzzle as libido let alone ED are multifactorial.
Getting quality sleep, minimizing stress (physical/mental), following a healthy diet, exercising/staying active, improving overall vascular health will have a far bigger impact than jacking up your trough FT!
Have realistic expectations especially when it comes to libido and erectile function
Now getting back to your FT also keep in mind that anyone with a TT 8-12 nmol/L or FT that falls between 5-10 ng/dL would be considered in the grey zone where many men can still experience low-T symptoms at such levels.
This is stated in some of the numerous testosterone therapy guidelines!
Any doctor in the know who is well versed in testosterone therapy that dealt with a patient that had a TT which fell in what would be considered the grey zone or better yet FT <10 ng/dL (100 pg/mL) along with symptoms of low testosterone would treat you.
Dr. Morgentaler who is considered the father of testosterone has treated 1000s of men over decades has stated numerous times that he would treat a man with a FT <10 ng/dL that was experiencing symptoms of low-T!
He would be considered top tier when it comes to (research/clinical experience) in the field!
If I were in your shoes seeing as your FT would easily be <10 ng/dL if tested using the most accurate assay (Equilibrium Dialysis) and I was experiencing symptoms of low-T then I would seek out a doctor well versed when it comes to treating low-T!
Final point that needs to be made here is I would not get too caught up on polymorphism of the AR/CAG repeat length (short/long) as testing for such is not available to the average joe let alone having a longer CAG repeat length is far from common!

Age-stratified reference ranges for directly measured (ED LC-MS/MS) serum free testosterone in healthy men
Just to be clear up any confusion this is Fiers camps data for mFT reference ranges not the harmonized reference range being worked on by the CDC. *Serum samples were analyzed from healthy men participating in the SIBLOS/SIBEX and EMAS studies, both population-based cohort studies * mFT...
*We established mFT reference ranges for healthy men aged 18 to 69 years
We present 95% mFT age-stratified reference ranges
Age category (years) | Median mFT (ng/dl) | 95% mFT reference range (ng/dl) |
18-29 (n=140) | 12.0 | 6.7-25.3 |
40-49 (n=207) | 8.1 | 4.3.14.2 |
50-59 (n=146) | 7.1 | 3.8-12.8 |
60-69 (n=126) | 6.4 | 3.4-11.7 |
70-79 (n=125) | 5.6 | 2.7-8.7 |
*The gold-standard for the determination of FT levels is considered to be directly measured free testosterone (mFT) using equilibrium dialysis followed by mass spectrometry (ED LC-MS/MS). However, no widely accepted reference ranges are available for this clinical parameter. We established mFT reference ranges for healthy men aged 18 to 69 years
*Serum samples were analyzed from healthy men participating in the SIBLOS/SIBEX and EMAS studies, both population-based cohort studies
* mFT levels were measured in 867 men using ED LC-MS/MS as previously reported (1).
Reference: 1. Fiers T, Wu F, Moghetti P, Vanderschueren D, Lapauw B, Kaufman JM. Reassessing Free-Testosterone Calculation by Liquid Chromatography–Tandem Mass Spectrometry Direct Equilibrium Dialysis. J Clin Endocrinol Metab. 2018;103(6). doi:10.1210/jc.2017-02360
In the current study, we used a state-of-the-art direct ED method to reassess FT in sets of representative serum samples. This method takes advantage of the ability of a highly sensitive and accurate measurement of T by liquid chromatography–tandem mass spectrometry (LC-MS/MS) to reliably measure the low FT concentration directly in the dialysate after ED. This more straightforward method avoids potential sources of inaccuracy in indirect ED, such as those resulting from tracer impurities or from measures to limit their impact (e.g., sample dilution). We then used the measured FT results to re-evaluate some characteristics of two more established and a more recently proposed calculations for estimation of FT.
Effect of Androgen Receptor Polymorphism on Hypogonadism Severity
*Average number of CAG repeats found was 23 ± 3.1, which is within the normal range as described by current literature * Half of the patients (n=8) had [EF] subscores
Again!
Yes there is such a thing as AR DDS (distribution, density, sensitivity/polymorphisms).
When it comes to sensitivity of the AR, polymorphism of the AR/CAG repeat length (long/short) tread lightly when you speak on such especially those pushing that everyone and their brother needing to run these very high/absurdly high trough FT levels 30-60 ng/dL in order to experience the beneficial effects of T!
Yes we are talking TROUGH f**king levels here!
Key point here having a CAG repeat length >24 is far from common!
* Based on a total sample of 57,826 males occupying 78 countries, the overall average number of AR CAG repeats was found to be 21.40. National averages ranged from 17.00 to 23.16.
*The same applies to androgen receptor gene CAG repeat lengths >24 in the presence of symptoms and normal testosterone levels may be considered as a state of preclinical TD [93]
Clinical implications of AR polymorphism in sexual health
https://academic.oup.com/jsm/article-abstract/20/11/1268/7334427?redirectedFrom=fulltext The androgen receptor (AR) plays a critical role in mediating the effects of testosterone on sexual development, libido, and sexual functions in men and women. Here with is an overview and opinion on the...
* Based on a total sample of 57,826 males occupying 78 countries, the overall average number of AR CAG repeats was found to be 21.40. National averages ranged from 17.00 to 23.16.
Variations in CAG Repeats of Men’s Androgen Receptor Gene
As the mediator of androgen actions, the androgen receptor (AR) plays a central role in establishing both physical and behavioral sex differences. The AR gene contains a CAG repeat polymorphism that is related to the strength of androgen actions on target tissues and that is correlated with...
*The same applies to androgen receptor gene CAG repeat lengths >24 in the presence of symptoms and normal testosterone levels may be considered as a state of preclinical TD [93]
*In humans, the AR gene comes in many forms, called alleles. The best-studied alleles are those involving a CAG repeat sequence that encodes a polyglutamine tract near the amino end of the androgen receptor. This CAG repeat has different lengths for different people. In humans, the number of AR CAG repeats ranges from as few as 9 to as many as 36, but population averages are typically between 17 and 24 (Chamberlain et al., 1994; Hsiao et al., 1999; Irvine et al., 2000; La Spada et al., 1991). Individuals with higher numbers of AR CAG repeats will normally have diminished testosterone action on cellular functioning, effectively making males with high AR CAG repeats less masculine regarding most sexually dimorphic traits when compared to males with fewer AR CAG repeats (Loehlin et al., 2004; Simanainen et al., 2011)
* Based on a total sample of 57,826 males occupying 78 countries, the overall average number of AR CAG repeats was found to be 21.40. National averages ranged from 17.00 to 23.16. Five countries had averages in the 17.00s; they were Swaziland (17.00), Zambia (17.00), Sierra Leone (17.30), Nigeria (17.58), and Senegal (17.90). Five countries had averages of 23.00 or higher; they were Lithuania (23.00), Mongolia (23.00), Ireland (23.07), Thailand (23.10), and Romania (23.16).
Testosterone Therapy (TTh) - How To Treat - Abraham Morgentaler
Have every lecture! Link to some of them. Excel is littered with AM! https://vimeo.com/user19492999
Low Testosterone in Men: Recommendations on the diagnosis, treatment and monitoring
ABSTRACT The relative proportional increase of the elderly population within many countries will become one of the most significant social transformations of the twenty-first century and, for the first time in history, persons aged 65 or above outnumbered children under five years of age...
AR CAG repeat lengths (short/long)
*The number of cytosine–adenine–guanine triplet (CAG) repeats in androgen receptors differ in men and influences the androgen receptor activity [88,89,90,91] (Figure 1). Hence testosterone sensitivity may vary in different individuals.
*The same applies to androgen receptor gene CAG repeat lengths >24 in the presence of symptoms and normal testosterone levels may be considered as a state of preclinical TD [93]
*In general, it is currently speculated that variable phenotypes of androgen insensitivity exist, mainly owing to mutated androgen receptors. More subtle modulation of androgen effects is related to the CAG repeat polymorphism in exon 1 of the androgen receptor gene: transcription of androgen-dependent target genes are attenuated with the increasing length of triplets.
*As a clinical entity, the CAG repeat polymorphism can relate to variations of androgenicity in men in various tissues and psychological traits: The longer the CAG repeat polymorphism, the less prominent is the androgen effect when individuals with similar testosterone concentrations are compared.
*A strictly defined threshold to TD is likely to be replaced by a continuum spanned by genetics as well as symptom specificity. In addition, the effects of externally applied testosterone can be markedly influenced by the CAG repeats and respective pharmacogenetic implications are likely to influence indications as well as modalities of testosterone treatment of hypogonadal men. Investigation of CAG repeat polymorphism in exon 1 of the androgen receptor gene may be useful in testosterone treatment regimens adjustment
Highly cited paper here!
Eye opener for many!
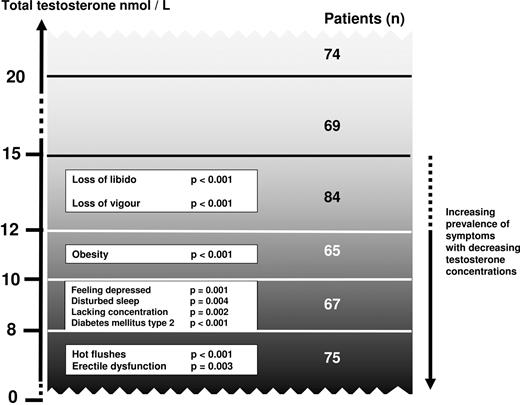
Association of Specific Symptoms and Metabolic Risks with Serum Testosterone in Older Men
Abstract. Context: Although attention and concern about health disorders in aging men have been growing, the structure of psychological and somatic complai
 academic.oup.com
academic.oup.com
Androgen modulation of mesoprefrontal dopamine systems and the effects of these actions on the adult male brain
Again would tread lightly on how high you run your trough/steady-state FT level! This can easily backfire in the long-run for many especially when it comes to mood, libido and erectile function! Too high a FT level can be just as bad in many ways as having too low a FT level. Libido starts in...
Libido starts in the brain.
Neurotransmitters have a big impact especially dopamine.
There is a fine balance here when it comes to the dopamine system!
This is key here..... dopamine circuits are powerfully regulated by androgens!
*dopamine circuits are powerfully regulated by androgens
*androgens as potent modulators of prefrontal cortical operations and of closely related, functionally critical measures of prefrontal dopamine level or tone
*androgens dynamically control meso prefrontal dopamine systems and impact prefrontal states of hypo- and hyper-dopaminergia
*dopamine-dependent prefrontal operations appear to universally follow inverted U shaped functions
* androgens maintain a lifelong capacity to bidirectionally modulate prefrontal dopamine tone
*By targeting enzymes and signaling molecules associated with androgenic metabolites of testosterone (Fig 1), these studies more directly implicate androgens in modulating prefrontal function. They also show that both supranormal androgen stimulation and androgen deficiency negatively affects prefrontal operations (Fig 2A). This inverted U- shaped function is similar to that described for functional meso prefrontal dopamine settings (Cools R and D'Esposito M, 2011; Cools R et al.,2019; Floresco SB, 2013; Floresco SB and Magyar O, 2006)
*The data also demonstrate an inverted U-shaped function that describes these dopamine effects. According to this function, prefrontal dopamine levels— often referred to as prefrontal dopamine tone- that are either higher or lower than a functionally optimal set point are detrimental to behavior and circuit function (Fig 2B).
Look over the threads in post #3
Truth About Testosterone and Your Libido
https://www.yahoo.com/lifestyle/truth-testosterone-libido-185000725.html?soc_src=social-sh&soc_trk=tw&tsrc=twtr As an expert on andrology and sexual dysfunctions, urologist Andrew Y. Sun, M.D., sees plenty of patients who’re struggling with low libido. And most are pretty sure they already...
*The male sexual response cycle is complex and the exact role of testosterone in mediating libido, arousal, erection, ejaculation, and orgasm is multifactorial
*This hormone isn’t the only biological factor with clear, substantial power over our libidos
Everything is perfect except low libido
Started test 6 weeks ago. I feel great. Good sleep, good training, feeling good and so on. Was at 140 mg test and 500 iu hcg every week (EOD shots). I started to feel some pain in the chest and did a fast blood test to only check test and estradiol. Came back at 48nmol/l and 0.17 nmol/l (Do I...
*Again having a healthy FT is only one piece of the puzzle as libido let alone ED are multifactorial.
*Getting quality sleep, minimizing stress (physical/mental), following a healthy diet, exercising/staying active, improving overall vascular health will have a far bigger impact than jacking up your trough FT!
*Have realistic expectations especially when it comes to libido and erectile function!












