Probably it would take at least three weeks to stabilize with enanthate, and a similar amount or a few days more with cypionate, using half-lives of 4.5 and 5 days respectively.Thanks @Cataceous...
Last question, in terms of the enanthate/prop mix.. I'm assuming it would take much longer to stabilise on this protocol vs the phenylpronionate due to the much longer half life of the enanthate? What would you theorise is a sensible way of moving to this mix from daily subq 10.5mg prop, minimising sides expected from such a transition?
Intuitively, I like the idea of controlling the trough levels with enanthate and merely adjusting for peak and variation with prop. Thanks
NB: when I say mix, I'm referring to your current prop daily and enanthate EOD protocol
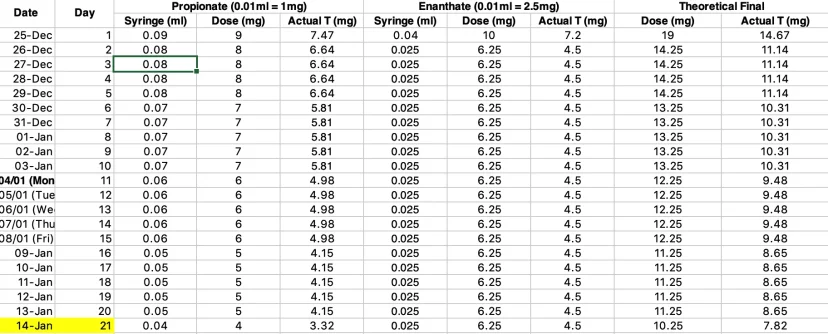
For a really gradual transition off of only propionate I would immediately add the full dose of the second ester, e.g. enanthate, and then gradually taper the propionate dose so that after two weeks +/- it's at the desired long-term level. I didn't bother with this procedure during my transition—I just went immediately to final doses, which presumably led to drop in average levels followed by a buildup over the next few weeks. If there were side effects from this they were too subtle for me to notice. It might be different when moving to a higher percentage of the longer ester, where you'd be more likely to see hypogonadal-type levels in the beginning.
An alternative approach is to front-load the longer ester. You inject a large dose upfront, equivalent to what would be present in you if you were already at steady state. Then you can immediately reduce the propionate dose.

 I just finished some part time studying while working and if it was not for 'modafanil' I would have been overtaken by the fatigue. Stopped taking modafanil and the lethargy associated with protocol etc. has returned. It's like I'm a different person - dont' care for much, taking it too easy etc.
I just finished some part time studying while working and if it was not for 'modafanil' I would have been overtaken by the fatigue. Stopped taking modafanil and the lethargy associated with protocol etc. has returned. It's like I'm a different person - dont' care for much, taking it too easy etc.