@Cataceous @readalot @Nelson Vergel
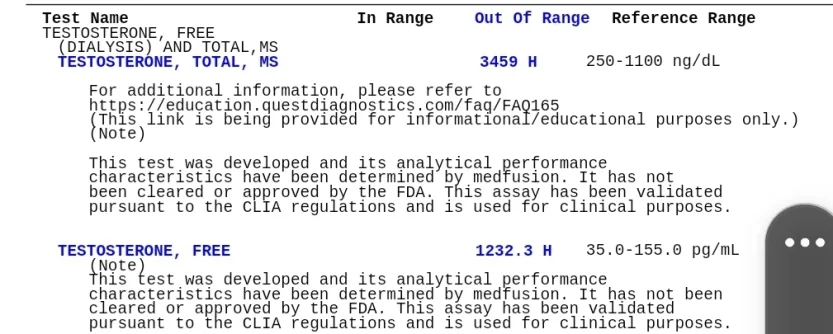
I got the labs back from Monday...keep in mind this is still 5mg on average. So sometimes a little closer to 6 and sometimes a little closer to 4 since there's no line for 5mg. 3459 was my total testosterone and 1232 was my free testosterone! Below are the labs and ranges.
Quest Diagnostics
10mg daily trough, total T, MS 550 (250-1100) 6 weeks
10mg daily 5 hours post, total T, MS 664 (250-1100) 9w
10mg daily...3 weeks
7mg daily...no test 4w
5mg daily trough, total T, MS 414 (250-1100) 2w
5mg daily trough, total T, MS
3459 (250-1100) 2w
For reference, below are the free testosterone results corresponding with the above dose.
Quest Diagnostics Dialysis
10mg daily trough, 147 (35-155)
10mg daily trough, 174 (35-155)
5mg daily trough, 105 (35-155)
5mg daily trough,
1232 (35-155)
As previously mentioned, I only changed my type of b12 and dropped telmisartan, dhea and the multivitamin. I promise to all of you this is the real results. What do I do? Is this an error? Do I have to pay to get it redrawn?
Is there a chance that previously the methylcobalamin and methylfolate increased methylation so fast that's why I was dropping my levels so rapidly day to day? I realize this is a stretch but I don't know what else to think. I've shown Cataceous my labs where my test levels dropped 50% in 24 hours when I was on EOD.
If this is accurate, how long until my levels are back to where they should be if my last injection was Sunday morning, 3/27?
Also, regarding the military/VA labs. These results were drawn 5 days before my astronomical testosterone results from Quest above. Those results are below:
Testosterone, total 766 (158-768)
Testosterone, Free 11 pg/mL (8-25)
More reason to believe the Quest results are an error?
Thanks in advance.





















")
