Here is another study I found I wanted to add to this discussion
Shalender Bhasin,
Effects of Testosterone Administration on Fat Distribution, Insulin Sensitivity, and Atherosclerosis Progression, Clinical Infectious Diseases, Volume 37, Issue Supplement_2, September 2003, Pages S142–S149,
Effects of Testosterone Administration on Fat Distribution, Insulin Sensitivity, and Atherosclerosis Progression
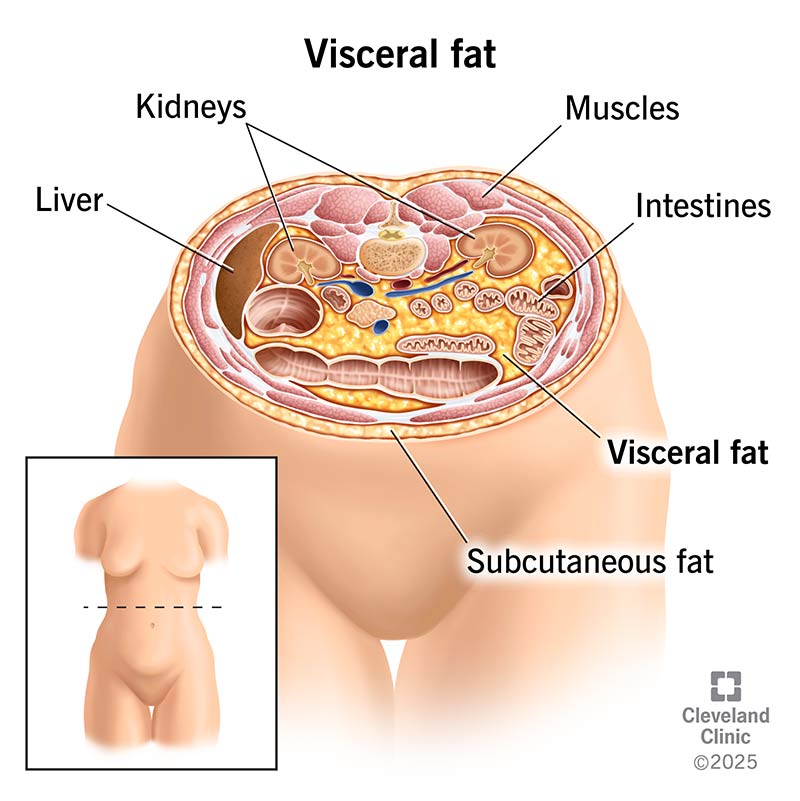
Testosterone administration to middle-aged men is associated with decreased visceral fat and glucose concentrations and increased insulin sensitivity. Testosterone infusion increases coronary blood flow. Similarly, testosterone replacement retards atherogenesis in experimental models of atherosclerosis.
Effects of Testosterone Administration on Fat Distribution, Insulin Sensitivity, and Atherosclerosis Progression
Plus this earlier study:
Atam B. Singh, Stanley Hsia, Petar Alaupovic, Indrani Sinha-Hikim, Linda Woodhouse, Thomas A. Buchanan, Ruoquing Shen, Rachelle Bross, Nancy Berman, Shalender Bhasin,
The Effects of Varying Doses of T on Insulin Sensitivity, Plasma Lipids, Apolipoproteins, and C-Reactive Protein in Healthy Young Men, The Journal of Clinical Endocrinology & Metabolism, Volume 87, Issue 1, 1 January 2002, Pages 136–143,
Effects of Varying Doses of T on Insulin Sensitivity, Plasma Lipids, Apolipoproteins, and C-Reactive Protein in Healthy Young Men
To determine the effects of different doses of T, 61 eugonadal men, 18–35 yr of age, were randomly assigned to 1 of 5 groups to receive monthly injections of long-acting GnRH agonist to suppress endogenous T secretion and weekly injections of 25, 50, 125, 300, or 600 mg T enanthate for 20 wk. Dietary energy and protein intakes were standardized.
Over a wide range of doses, including those associated with significant gains in fat-free mass and muscle size, T had no adverse effect on insulin sensitivity, plasma lipids, apolipoproteins, or C-reactive protein. Only the highest dose of T (600 mg/wk) was associated with a reduction in plasma high density lipoprotein cholesterol and apolipoprotein A-I.
Effects of Varying Doses of T on Insulin Sensitivity, Plasma Lipids, Apolipoproteins, and C-Reactive Protein in Healthy Young Men
Insulin
The effects of T administration on glucose metabolism and insulin sensitivity remain poorly understood. Total T levels are inversely related to insulin concentrations in several cross-sectional studies (
39,
42–
45). Fasting insulin levels are higher and T and SHBG values are lower in men with type 2 diabetes mellitus (
39). Haffner
et al. (
39) reported that lower T levels were correlated with a higher waist/hip ratio and lower nonoxidative, whole body glucose disposal in men.
Administration of exogenous androgens has been reported to induce glucose intolerance and hyperinsulinemia in some studies (20–22), but other studies found no significant changes in glucose tolerance or insulin concentrations with administration of T or 19-nor-T to men even at pharmacological doses (46). A marked lowering of T levels in the male rat by surgical castration as well as the administration of supraphysiological doses of T induces insulin resistance (
20). This suggests that the relationship between T levels and insulin sensitivity might be curvilinear. Our study failed to find any significant changes in SI, SG, and AIRG in any treatment group over a wide range of serum T concentrations. Our data differ from those of Marin (
17–
19,
47), who reported improvements in insulin sensitivity, blood glucose, and blood pressure after T supplementation in middle-aged men who had visceral obesity and low T levels. In contrast to the studies by Marin
et al. (
17–
19,
47), the subjects in our study were younger and had significantly lower fat mass. Marin
et al. used euglycemic-hyperinsulinemic clamp, whereas we used frequently sampled iv glucose tolerance test to assess insulin sensitivity; we do not know whether the differences in methodology could have contributed to the observed differences in outcomes.
We cannot exclude the possibility that in middle-aged men with midsegment obesity, T might decrease whole body and intraabdominal fat and thereby improve insulin sensitivity.
Here is another relevant study on muscle mass and gynoid fat or fat around the hips, thighs and chest areas.
Cite
- Nordström, Anna; Högström, Gabriel; Eriksson, Anders; Bonnerud, Patrik; Tegner, Yelverton; Malm, Christer. Higher Muscle Mass but Lower Gynoid Fat Mass in Athletes Using Anabolic Androgenic Steroids. Journal of Strength and Conditioning Research 26(1)
 246-250, January 2012. | DOI: 10.1519/JSC.0b013e318218daf0
246-250, January 2012. | DOI: 10.1519/JSC.0b013e318218daf0
Thus, long-term AAS use seems to alter body constitution, favoring higher muscle mass and reduced gynoid fat mass without affecting BMD (bone mass density).
Intake pattern was examined through extensive interviews and questionnaires. Ten of the athletes had used various AAS substances such as testosterone (oral and injectable anabolic steroids [250–2,000 mg·wk−1]), dianabole (Methandrostenolone, oral anabolic steroid [50–350 mg·wk−1]), deca-durabolin (Nandrolone Decanoate, injectable anabolic steroid [200–7,000 mg·wk−1]), boldenone (Boldenone undecylenated, injectable anabolic steroid [500–1,000 mg·wk−1]), and anadrol (Oxymetholone, oral anabolic steroid [175 mg·wk−1]) and also substances such as insulin (injected [10–12 IU·d−1]), insulin-like growth factor-1 (injectable growth protein [50 mg·d−1]), GH (Growth Hormone, injected [4–6 IU·d−1; 6 d·wk−1]), Ephedrine (oral appetite suppressor [60 mg·d−1]) and HCG (human chorionic gonadotropin, injectable glycoprotein hormone [10,000 IU total]). The substances had been used in different combinations and doses for a period of 5–15 years; thus, the exact doses are not possible to determine.
Again, I am not fond of the term "abuse" or "doping."
But this study concluded: Increased percent lean body mass and decreased adipose tissue appear to be a result of long-term AAS abuse.